It can't happen to me
When I go back to Asia, including Taiwan, it is to attend national symposium conferences, where I go and help educate the scientists and the physicians in those countries. But I worry about the perceptions of the public. From my contact with relatives and friends in Taiwan, I have found that there is a general attitude that this won't happen to me. This is not my problem. This is your U.S. problem, your African problem, your Thai problem. This is your homosexuals' problem and drug users' problem. This will not happen to me. It was that kind of attitude that prevailed in the U.S. early on in the epidemic. The result was that ten years later, 1.5 million people were infected. If you want to prevent AIDS, the first thing is to get rid of the it-can't-happen-to-me attitude.
How can you develop strategies together as a nation? The best thing to do is to educate everyone in the population, old and young. It is clear how AIDS is transmitted: almost 90 percent by sex. And no matter what you tell them, people are still going to have sex. In Asian countries, sex is still a forbidden subject. But for reasons of public safety, governments and the media are duty bound to spread the word.
The virus vs. the antibody
Q: Can you briefly explain to our readers how HIV can remain dormant in the human body and what triggers full-blown AIDS?
A: Actually there is some revision in that story. It is no longer believed that the AIDS virus lays completely dormant in the cells.
So a person gets infected at time zero. About a few weeks later the virus grows to a very, very high level. Then within a short period of time it comes down. We think this is an effective immune reaction to the disease. This controls it to a rather good degree. That stage is what we call the clinical latency period. That is when it appears to be clinically dormant. But from studying it carefully, we know it is not completely dormant. The virus is still replicating, except that the level is very low. And for many years it is a constant struggle between virus and host. We have individuals who after 15 years are still doing very well. But on average, sometime between years seven and ten, the virus begins to win and the immune system declines.
What allows the virus to win is its ability to change. Some of the changes will result in viruses that grow faster, a virus that kills the cells better, or a virus that has changes in the outer surface of the virus so that it is no longer recognized by the immune system. It gradually gains the upper hand in the body, takes over.
Technically speaking, the virus never lays completely dormant. It only appears to do that. I do not think there is a viral latency period, only a clinical latency.
Another AIDS-like disease has received a lot of publicity. Yet we are talking about tens of cases, while there are millions of real AIDS cases. So we should not divert too much of our attention from the real AIDS epidemic to something that could turn out to be a rather minor clinical disease. But if there is a real entity that is due to a virus similar to HIV, then it becomes important. We certainly want to prevent a second epidemic. It would be tragic if we missed that. Again it is a balancing act. We have studied 17 of these patients to date. We are working very hard to see if we might come up with something.
I want to emphasize that we've got to pay more attention to the actual AIDS virus. Take Thailand. In a matter of four or five years the number of cases there went from almost nothing to over half a million. That is frightening.
Later or earlier--a matter of luck?
Q: Sometimes the virus wins early, sometimes late. Why is that?
A: We do not know. This is one of those very, very important central questions in AIDS research. You can say one person gets a virus that is worse than another person's virus because there are strain to strain variations. We also know that the immune system and the susceptible cells within the host are different. Some patients respond better than others. In addition we think there may be a matter of luck also. By that I mean it is a more or less random process where the virus mutates.
For one individual the mutations may be benign or silent, whereas for others, the mutations--say in the surface coat of the virus--could result in it escaping the immune system or result in a virus that grows faster. Scientifically, this is called a stochastic process, a fancy way of saying luck.
Q: Isn't there a new AIDS-like virus which has of late been in the public spotlight? At an international conference on AIDS in Amsterdam, you made a research report about this new virus. Could you talk about the latest research results?
A: It is really unclear right now. There are clearly patients out there who have abnormal immune systems. Some of these abnormalities in the immune system are very similar to the abnormalities of AIDS. But it is also very clear that they do not have HIV infection. Those patients exist. The question is, are they caused by one process, one virus or something? We don't know. If you put all the cases together, it is not clear that all of these fit into one syndrome.
Resorting to sensationalism?
Q: People are most afraid of the safety of having blood transfusions. Not long ago someone in Ohio who had previously arranged to have his organs given away when he died was killed in an accident. The result was that he gave AIDS to the people who received his organs even though tests before donation had said that he wasn't carrying the virus.
A: Testing in general is very good. But there is a clinical situation where testing could miss a case of infection. This is during the very early part of HIV infection, during the first few weeks of infection. The antibodies that are made to combat the virus are not produced until a few weeks later. So you have a window period when a person has the virus, sometimes a high level of the virus, but no antibodies [Ed note: HIV is actually detected by screening for these antibodies rather than for HIV itself.].
But it has been estimated that in the U.S., with screening programs in place, there may be only a dozen or few dozen cases that have occurred because of this window period despite the large number of individuals infected. Given the lower prevalence of HIV infection in the Taiwan population, the risk should be even less. The odds of getting it are smaller than getting the lottery.
Q: If chances of getting AIDS through receiving blood is so low, as long as one handles one's life--strictly speaking, one's sex life--properly, shouldn't there be next to no risk of getting the virus? Isn't this talk about its being everyone's problem a bit sensationalistic?
A: It's true if you handle your sex life properly, you probably don't have to worry about the virus. But as the number of infected grows, even if you don't get it yourself, some of the people around you may. It's a matter of time.
I have seen many cases of such individuals. Many of them are kept well-hidden and you don't hear about them because people prefer to keep their privacy. I can tell you with great certainty it is spreading into families you normally would not suspect.
A hard search for a vaccine
Q: The treatments now being tested, even if they are successful, are going to be very expensive--more than what most people can afford.
A: Yes. Although cost is a consideration in designing treatment methods, a high cost is often unavoidable. It is just like the early days of dialysis. When you have the dialysis machines to save patients from kidney failure, do you only do it for those who can afford it or do you do it for everybody? I think if that is the way things develop, then there should be a national policy. But in the end, the rich always get better care.
Q: A vaccine is the best method for preventing the spread of a disease. How is research going in this respect?
A: We are trying to study proteins on the surface of HIV, trying to attack it with immune system antibodies or with cell responses, certain types of killer cells or cytotoxic cells that would attack the virus itself or virus-infected cells. The old approach is just to make the vaccine from the whole virus by killing it and showing it to the immune system. That was how the polio vaccine was made. These are called heat-inactivated or killed-whole-virus vaccines. As the technology has gotten more sophisticated, you can make a virus just out of the surface protein. You don't need the rest of it. Just like for the massive immunization for hepatitis B in Taiwan right now. AIDS research is basically taking this route.
Strange beasts in the forest
For HIV it is going to be harder because there is so much strain to strain variation. The surface protein from one strain looks different from another. Yet there are enough conserved features for the virus to do its thing. So there are some conserved regions of the protein, and yet there are variable regions of the protein, and the immune system is somehow tricked to make antibodies. So our whole approach is to figure out the structure and function of the glycoprotein, the protein on the surface, so that we know which part is important to the virus and which parts are not.
It is like you are running in the jungle with a rifle. A strange animal shows up. An animal you have never seen before. You only have one shot to fire. You don't want to end up hitting its tail unless you know the tail is important. You want to figure out where the targets are before firing. So our work right now is very basic. We are not ready to make a vaccine.
But there are a lot of groups taking the old approach, taking the whole virus. Based on animal testing so far, it does not look like these will be successful. You can get successful results in the animals with some of these approaches but ultimately they are not going to work in a human population with many, many different strains of HIV. So there is still a long way to go. I do not think a broadly efficacious vaccine will be available in three to five years.
[Picture]
p.126
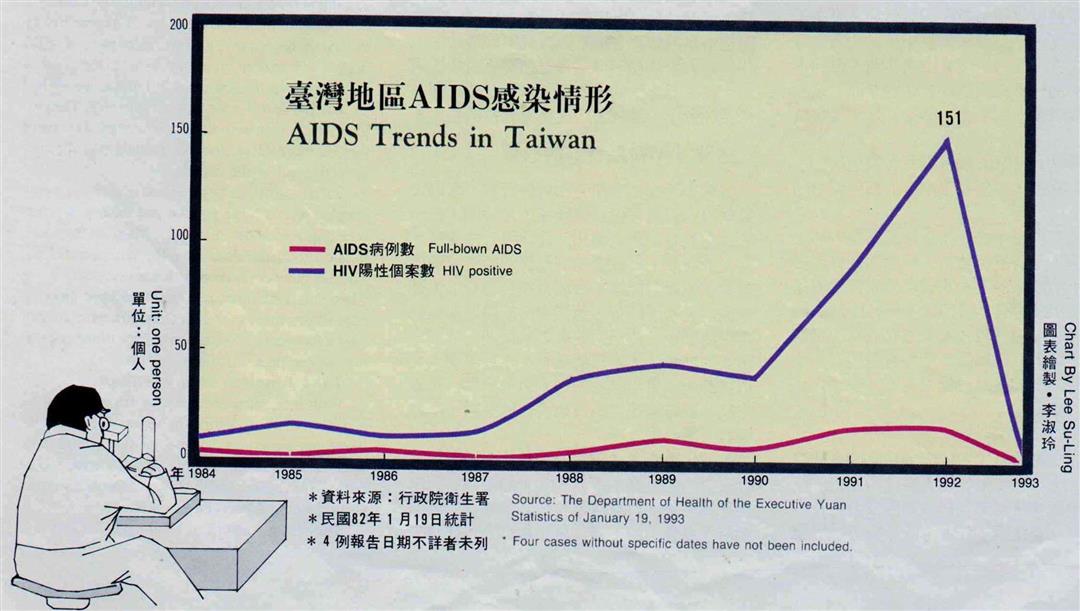
AIDS Treds in Taiwan
Source:The Department of Health of the Executive Yuan
Statistics of January 19,1993
Four cases without specific dates have not been included.
p.127
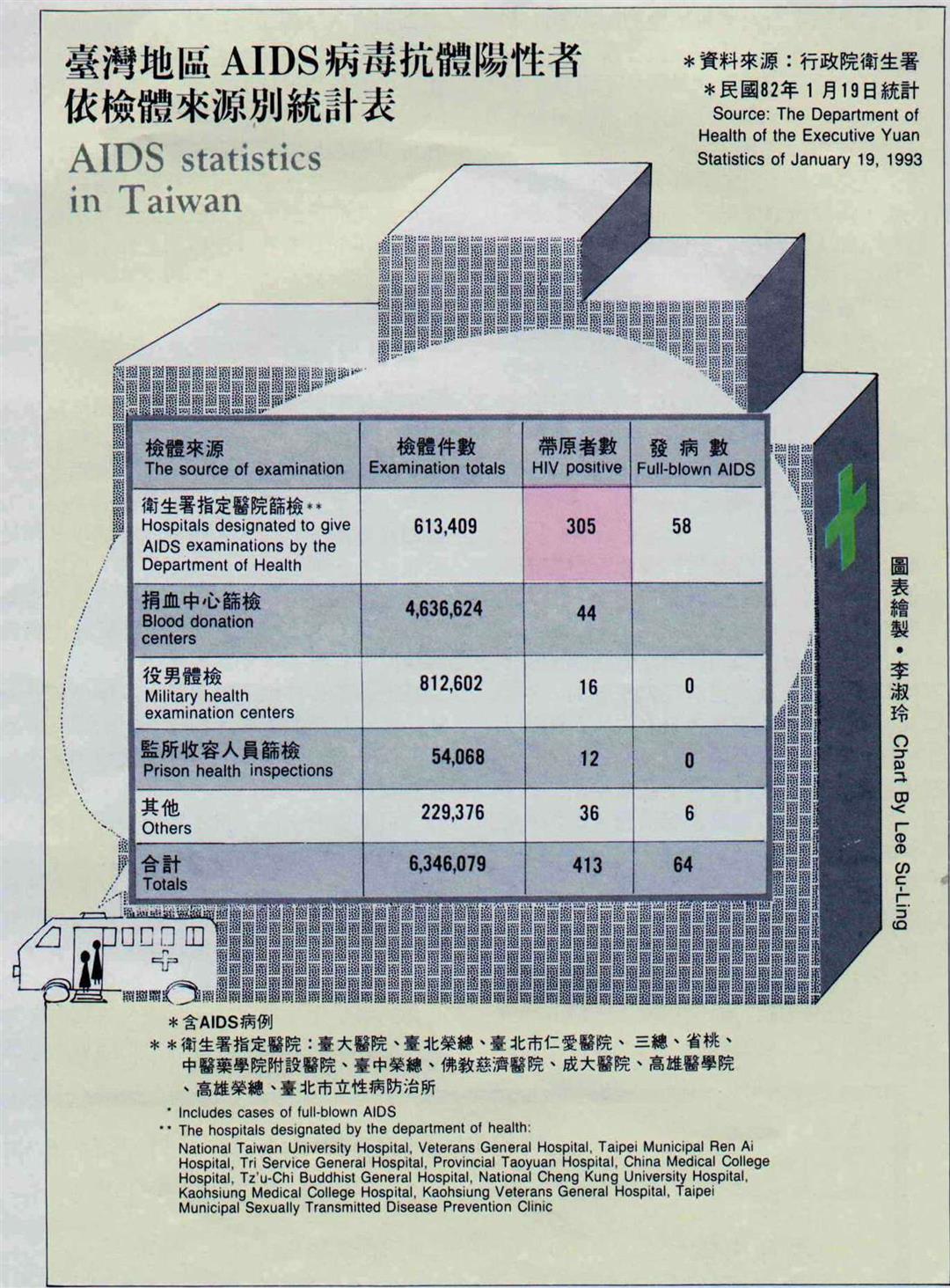
AIDS statistics in Taiwan
Source:The Department of Health of the Executive Yuan Statistics of January 19,1993
Includes cases of full-blown AIDS
The hospitals designated by the department of health:
National Taiwan University Hospital, Veterans General Hospital, Taipei Municipal
Ren Ai Hospital, Tri Service General Hospital, Provincial Taoyuan Hospital, China Medical College Hospital, Tz’u-Chi Buddhist General Hospital, National Cheng Kung University Hospital, Kaohsiung Medical College Hospital, Kaohsiung Veterans General Hospital, Taipei Municipal Sexually Transmitted Disease Prevention Clinic
p.128
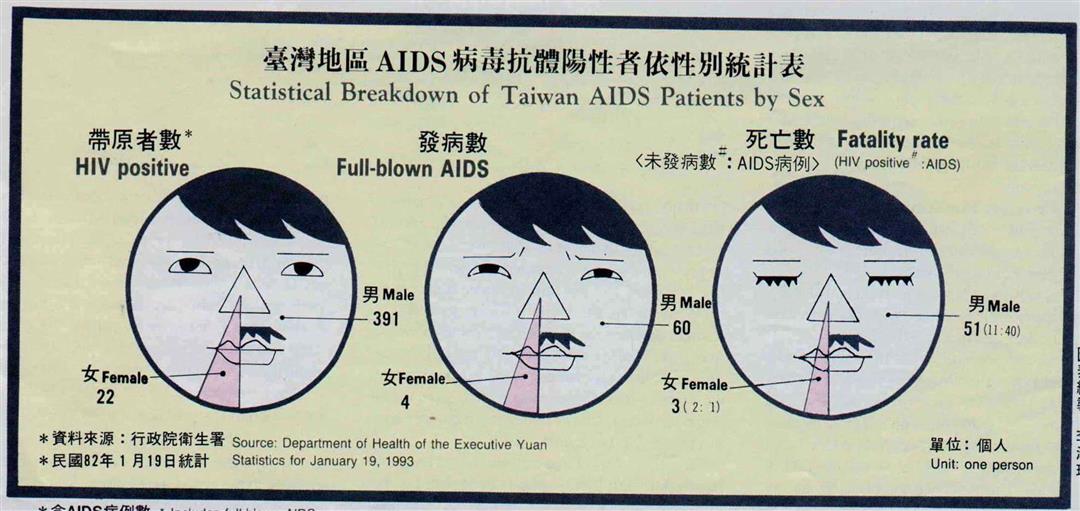
Statistical Breakdown of Taiwan AIDS Patients by Sex
Source:Department of Health of the Executive Yuan
Statistics for January 19,1993
Includes full-blown AIDS
The reasons people who did not yet have full-blown AIDS died include accidents, suicide and other diseases(such as hepatitis and kidney failure)
p.129
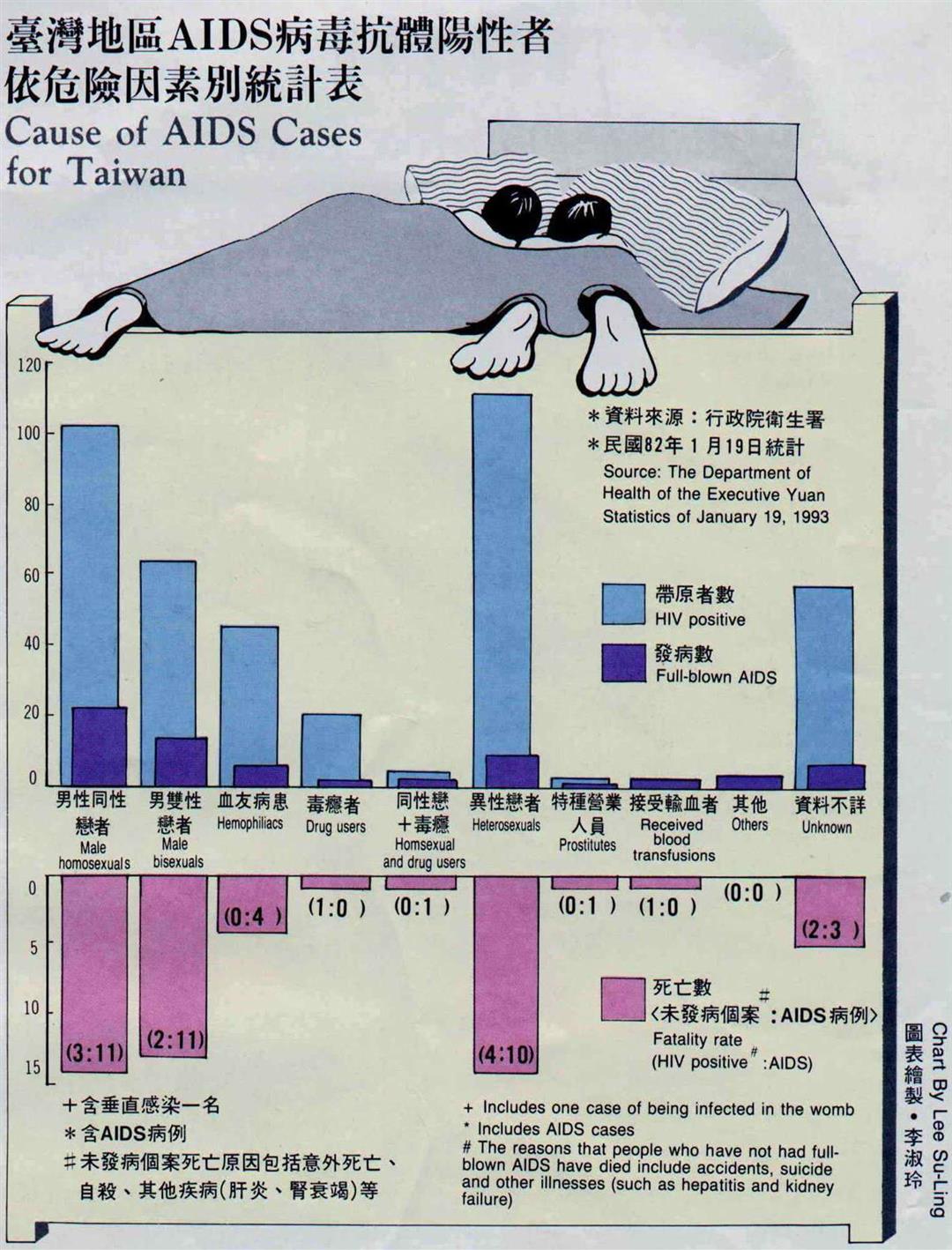
Cause of AIDS Cases for Taiwan
Source:The Department of Health of the Executive Yuan Statistics for January 19,1993
Includes one case of being infected in the womb
Includes AIDS cases
The reasons that people who have not had full-blown AIDS have died include accidents ,suicide and other illnesses(such as hepatitis and kidney failure)

@List.jpg?w=522&h=410&mode=crop&format=webp&quality=80)
@List.jpg?w=522&h=410&mode=crop&format=webp&quality=80)




