If you drew up a list of protest activities in Taiwan over the past year, after political and environmental protests, actions taken over the labor insurance problem would probably rank third. About seven million people in Taiwan are eligible for labor insurance; thus the impact of the system is profound.
Last July, 95 middle and small scale clinics in Nantou county which were contracted to handle patients under labor or farmers' insurance announced they would go on strike to force the Bureau of Labor Insurance to push forward the implementation of new standards for compensation. Overnight, doctors' associations across the province added their support. To put it simply, it's all about money.
Under intense scrutiny, parts B and C were implemented early, in November, as the advocates desired. As of today the A part will be implemented on July 1. So now it is the turn of the big medical centers to object.
The larger centers who come under the A schedule received the final plan on May 11. After some calculations, they discovered that the new plan lowered compensation by 10-20% compared to the old scheme. Some items even required the hospitals to operate at a loss. As a result, a rebellion began brewing.
In the face of objections, Bureau of Labor Insurance Director General Chang-feng Lin noted that, "With the pie for medical care so huge, everyone thinks to get a slightly larger share, but differences arise over what distribution is both rational and proper."
When labor insurance was first implemented in 1979, the system used was that hospitals would first report the number of cases handled and then be compensated accordingly. Further, larger units with better equipment would negotiate with the Bureau of Labor Insurance one by one their compensation standards. This led to a large gap in compensation between large institutions and small and medium clinics, sometimes reaching 500-600%.
This compensation differential created a bias in the public. Larger hospitals were more openhanded with treatment and medication, so that people competed to stay in those.
"This situation of large hospitals having to constantly expand to meet the huge number of patients and small hospitals shrinking, or even cheating in order to 'live off of labor insurance' is a major factor leading to the mass protests by small and medium clinics," points out Liu Chien-hsiang. But the victims are not only the clinics.
In order to resolve these problems, the ABC schedule has two key principles. One is "same illness, same compensation." When hospitals of whatever size treat the same illness, the methods should be similar, so compensation naturally will be similar. The "classification of treatment" principle divides illnesses into A, B, and C classes according to difficulty of treatment. Large hospitals treat the tougher problems, small clinics the lesser ones.
"Simply put, this is a change in the structure of labor insurance payments," says Lin Chin-lung, chief of the department's hospitalization section. Aside from eliminating a few types of payments to larger hospitals and redistributing them to smaller clinics, the former structure of payments according to medicine, equipment, and tests will be adjusted to be payment according to the services. The ABC program greatly reduces items for medicine and tests, and correspondingly raises doctors' examinations, surgery, room costs, and nurses' fees; it is hoped that this will raise the enthusiasm for service among medical personnel.
All this matters little to the larger institutions. The A schedule includes over 1000 items for serious illnesses that will force hospitals to take a loss. This will lower their willingness to accept seriously ill patients.
Chang-feng Lin believes that this is an apropos moment for hospitals to change operating principles. "In the past large hospitals just devoted themselves to expansion, and ignored management. Now that compensation is down, they will reorganize themselves, reduce waste, and strengthen management. Therefore lower payments are not necessarily without an up side."
Unfortunately, the Bureau of Labor Insurance is already paying out more than it takes in. The ABC plan will increase expenses by almost NT$8 billion. So the bureau has begun tapping the old age retirement account. However, in this year alone the bureau will come up NT$20 billion short in that fund, and "we still don't know where to go for the funding," worries Chang-feng Lin. Plans to make patients pay part of the costs of hospital visits have been frozen in the Legislative Yuan, and businesses have blocked plans to increase their contributions to labor insurance. But in the long term, "partial payment" and "increased contributions" are the only ways to resolve the crisis.
The point of insurance, Lin notes, is for everyone to spread the costs and risks of illness around to help the poor and disabled; the government cannot, nor does it have the duty to, provide unlimited subsidization. But to get a consensus on this idea won't be as easy as ABC.
[Picture Caption]
One little labor insurance slip has stirred up a storm of controversy in medicine on Taiwan.
Hospitals are pondering a dilemma: If they don't accept labor insurance patients, they lose business; if they do, they're afraid of losing money.
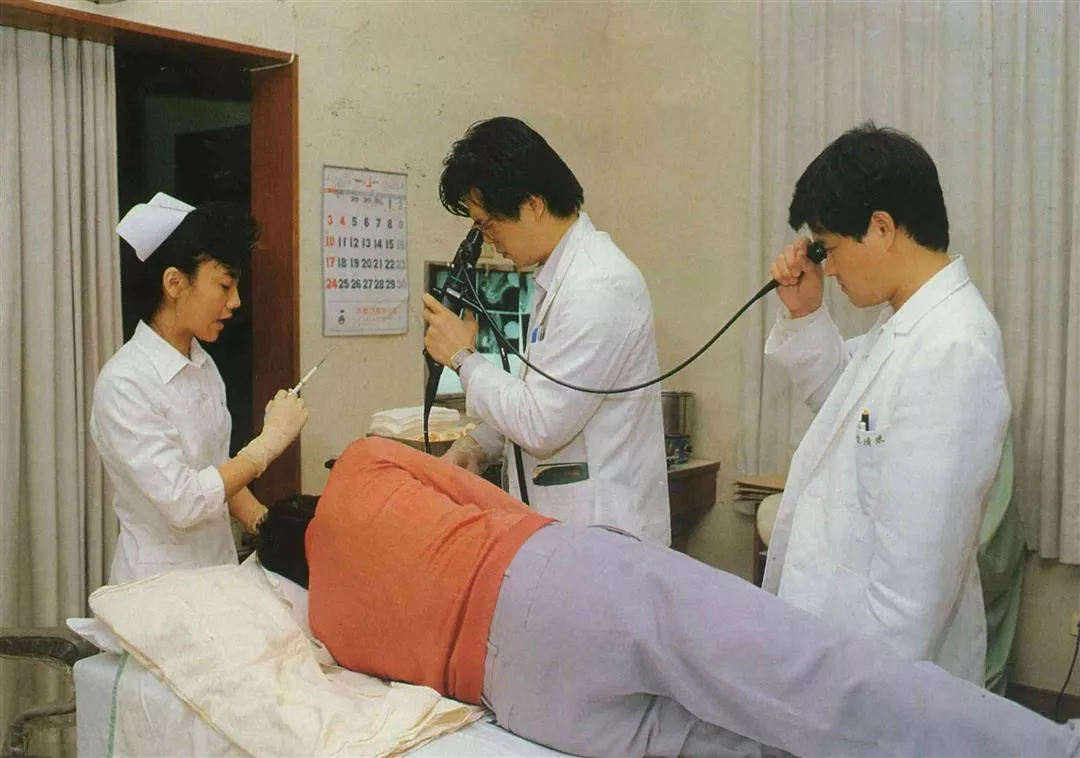
(Right) Larger hospitals receive greater payments from labor insurance, so the service is naturally better. (photo from Sinorama files)
(Above) Labor insurance patients prefer to go to large hospitals for treatment, even if it means spending more time waiting. (photo from Sinorama files)
(Below) Because of differences in the payment system, patients who have their teeth cleaned at a dental clinic may have to use three or four labor insurance slips t o cover the cost. (photo from Sinorama files)
The country is in urgent need of an adequate medical referral system.
The low level of payments for major illnesses under the A standards may lower the willingness of doctors to perform orthopaedic and cerebral surgery. (photo by Arthur Jeng)
Will expensively equipped hospital rooms be out of the reach of labor insurance patients if the payments are too low?
The Chinese habit of overusing medicines places a heavy burden on the labor insurance system.
Hospitals are pondering a dilemma: If they don't accept labor insurance patients, they lose business; if they do, they're afraid of losing money.
(Right) Larger hospitals receive greater payments from labor insurance, so the service is naturally better. (photo from Sinorama files)
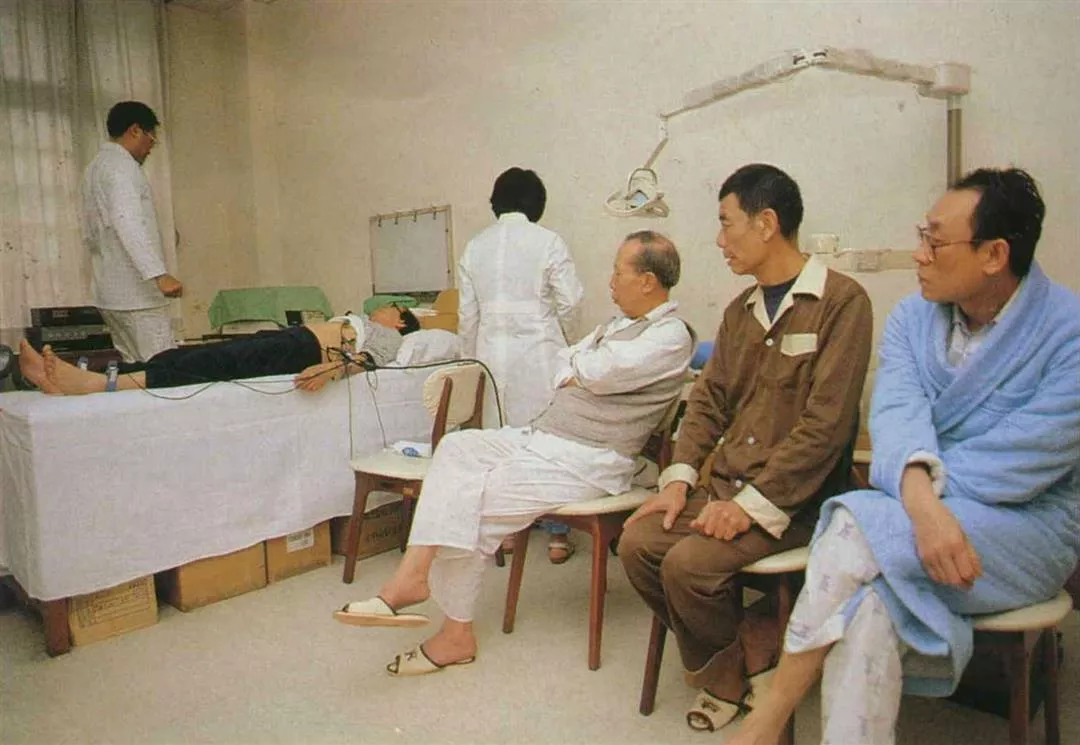
(Above) Labor insurance patients prefer to go to large hospitals for treatment, even if it means spending more time waiting. (photo from Sinorama files)
(Below) Because of differences in the payment system, patients who have their teeth cleaned at a dental clinic may have to use three or four labor insurance slips t o cover the cost. (photo from Sinorama files)

The country is in urgent need of an adequate medical referral system.
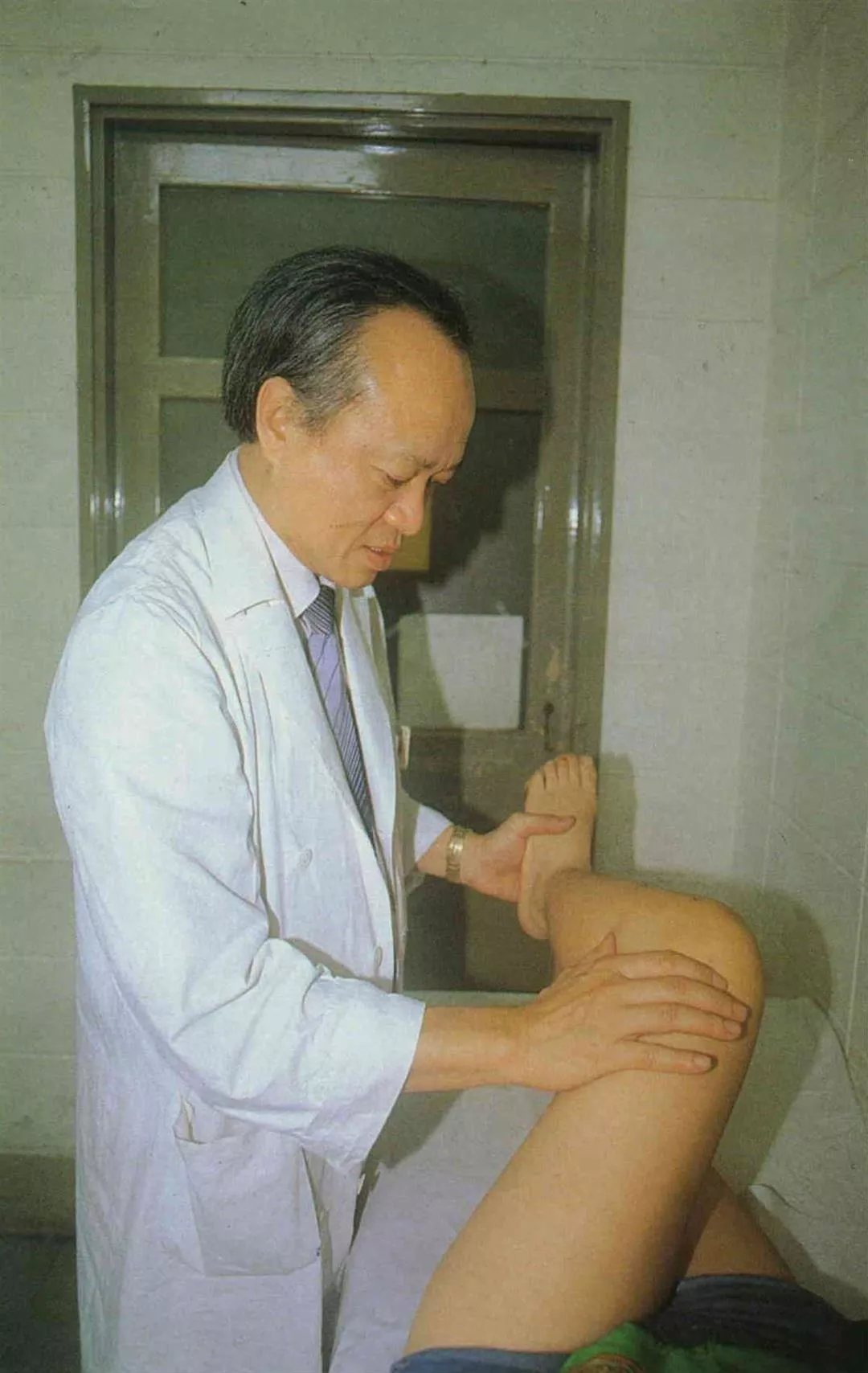
The low level of payments for major illnesses under the A standards may lower the willingness of doctors to perform orthopaedic and cerebral surgery. (photo by Arthur Jeng)
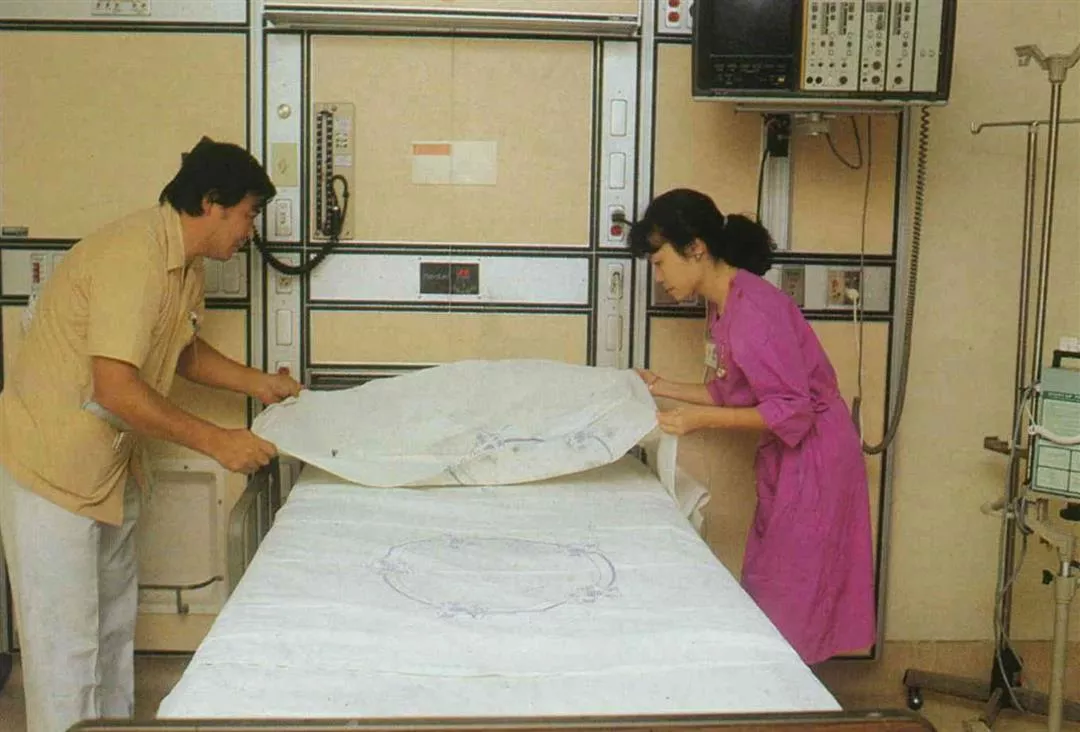
Will expensively equipped hospital rooms be out of the reach of labor insurance patients if the payments are too low?
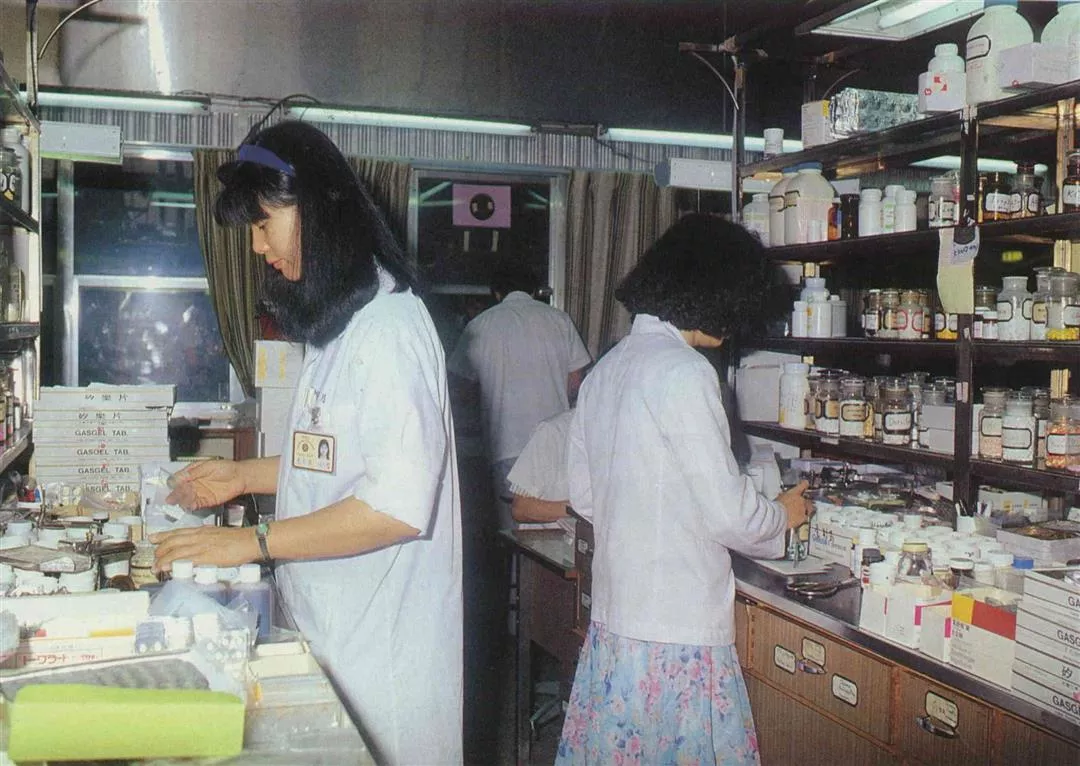
The Chinese habit of overusing medicines places a heavy burden on the labor insurance system.


@List.jpg?w=522&h=410&mode=crop&format=webp&quality=80)
@List.jpg?w=522&h=410&mode=crop&format=webp&quality=80)




@List.jpg?w=522&h=410&mode=crop&format=webp&quality=80)