ER doctors not only walk and talk fast, they virtually fly through their treatment of patients. But with the number of ER patients on the rise and less and less space in the ER, these doctors have no room to spread their wings. . . .
As we move into the winter, the ERs of Taipei's major medical centers are packed. In the ER of the National Taiwan University Hospital (NTUH), the beds of patients under observation are everywhere, spread all over the ER like the roots of a tree. Numbers are hung on the walls of the corridors. As soon as a patient is admitted, one need only place a bed under the next number and the patient has his bed space. But on the last day of a long weekend and over the Lunar New Year's holiday, the "high season" for ERs, when the numbers run out, "You even see a sign hung for the 'beside the laundry basket' spot," says Dr. Shih Fu-Yuan, a physician in the department of emergency medicine at NTUH.
A "clogged artery"
Even during the "off season," the ERs of Taiwan's major medical centers give one the impression of frenzied activity. There are the patients brought in by the emergency medical services, those who don't know which department they need to see, those in agonizing pain, the unconscious, those bleeding heavily, those in shock. . . everyone who is in critical condition or feels that they might be is there. And then there are those who are so ill that they really haven't the time or the strength to be admitted to see the hospital's doctors through the outpatient clinic.
Many patients whose condition is unclear remain in the ER for observation after they stabilize. When the nature of their problem becomes more apparent, they are moved into the ward, transferred to another hospital, or discharged. But the process is not usually as smooth as that.
In Taiwan, people tend to believe that the larger the hospital, the higher the quality of care, and there is a positive correlation between the quality of a hospital and the amount of crowding in its emergency room. Medical centers such NTUH and Linko's Chang Gung Memorial Hospital (CGMH) have had to expand their emergency facilities to address the problem of a never-ending stream of critically ill patients. But the larger those ERs become, the more inclined people are to go to them for treatment. It's a real Catch-22.
Dr. Michael Bullard, a consultant in emergency medicine at CGMH, has observed that not only are Taiwan's ERs packed with patients, they are also crowded with the family members of those patients. And most hospitals do not strictly control visiting hours or visiting areas. This leads to the ERs of major medical centers "resem-bl(ing) a traditional Chinese market," says Bullard.
Free sparring
ERs are open at all hours and, at least in theory, must treat each patient who registers, regardless of the relative severity of that patient's problem. This means that in addition to those critical patients needing urgent treatment, there are many people with non-critical ailments who come to the emergency room outside of outpatient clinic hours either because they don't want to wait for a doctor or don't have time during outpatient hours. "Many patients' reason is very simple: 'I'm in business and don't have time to come to the hospital,'" says Dr. Huang Ying-chieh, chief of emergency medicine at Chiayi Christian Hospital.
In addition, patients from small- and medium-sized hospitals with conditions that those hospitals are unable to treat are transferred to large hospitals. And those patients whose emergency care has been completed but don't yet have a bed in the ward are simply "checked in" to the emergency room itself. Taiwan's social welfare system is not fully developed and many patients who might otherwise be transferred to an organization like a convalescent home are instead left in the ER. Hence, the ERs of local medical centers are almost always full of patients.
Huang observes, "Taiwanese are very sensitive about 'face'; it sounds much better to say one's parents are staying at a major hospital than to say that they are in a convalescent home." Dr. Chang Kuo-song, director of the emergency department at Mackay Memorial Hospital, says that in the US, there are regulations which state that patients can only remain under observation in the ER for six to eight hours. In Taiwan, however, ER patients often stay in the ER for a week, and in some cases may even be there for as long as three months.
Not only do patients with conditions of all degrees of severity congregate in the ER, the ER is also often a temporary refuge for homeless drunks, elderly people without friends or family, abused children, rape victims and drug addicts. In the ER, seconds are critical to medical personnel dealing with life and death situations. Patients are anxious to be treated, but staff must nonetheless often resolve non-medical problems. There are therefore more conflicts within the ER than within any other hospital department. At CGMH a doctor was recently beaten so severely by a drunk patient that cerebrospinal fluid flowed out from his nose.
"By the time an ER patient is moved into the ward, his condition has already more or less stabilized and government and social organizations have already been contacted. At this point, 60% to 70% of the patients' problems have already been resolved by the ER," says Dr. Wang Lee-min, chief of emergency medicine at Veterans General Hospital.
Shih states that most critical patients' problems have appeared suddenly, and doctors have no way to predict what kind of problem their next patient is going to have. "It's like free sparring; you don't know what your opponent's next move is going to be," says Chang Kuo-song. But critically ill patients don't have much time. For a patient whose heart has stopped, there are four minutes before lack of oxygen causes irreversible brain damage. ER doctors must be able to restart a patient's respiration and pulse quickly, stabilize his condition and provide preliminary care.
The sight of blood
ER doctors must know something of every field of medicine as well as be able to resolve non-medical problems. Their abilities should, then, be exceptional. But in Taiwan, the opposite is often true.
In Taiwan, up until January of this year, emergency medicine was not an area of specialization as, say, internal medicine, surgery and dermatology are. Neither did it have a systematic organization. For many years, the doctors in the ERs of large local hospitals have been recently graduated residents who are still undergoing training in another department. These residents serve in the ER for a month or two before returning to their own departments.
Most of their training is in their own area, and modern medicine is very finely sub-divided into specialties. Surgery, for example, is sub-divided into eight or nine sub-specialties including cardiology and neurology. Dr. Tsai Ming-che, a physician in the ER of National Cheng Kung University Hospital, says that the division into secondary sub-specialties has allowed doctors to develop a very deep knowledge of their own area. But a seriously injured victim of a car accident or a fall may have injuries to the head, chest and abdomen. "What patients on the brink of death need is to have their vital signs stabilized and a complete evaluation. They can't wait for each specialist to take his time with an examination," says Dr. Huang Mu-shun, director of emergency medicine and traumatology at the Kaohsiung Veterans General Hospital.
The examination process of Taiwan's ERs has been described as, "If there's blood, send them to surgery. If there isn't, send them to internal medicine." Huang Ying-chieh elaborates on the examinations process, saying that in one case a mother whose son had had an asthma attack was bringing him to the hospital on a motorcycle when they were involved in an accident. When they finally arrived at the ER, the boy, who by now could barely breathe, was covered with injuries. "Then it depends on the doctor's skill. If the doctor weren't very good, he might begin by examining the wounds, ignoring the fact that the boy could barely breathe," says Huang Ying-chieh.
Establishing a specialty
Bullard observes that in recent years, with the emergence of cerebrovascular disorders, cardiovascular disease and accidental injury as three of the top 10 causes of death in Taiwan and the rise in the occurrence of accidents brought on by urbanization and industrialization, emergency medicine has been growing in importance.
To raise the quality of emergency care, the beginnings of an emergency medical discipline have been established in the last few years, meeting the calls of ER doctors for a professional certification. In 1989, Veterans General Hospital took the first step, proposing the island's first plan for the training of emergency medical residents.
Three years later, the Society of Emergency and Critical Care Medicine (SECCM) began certifications. But because the SECCM covers the fields of emergency medicine, critical care medicine and trauma surgery, some doctors of emergency medicine went further, establishing the Society of Emergency Medicine (SEM) in 1994 to focus on the development of emergency medicine and related academic research. This organization now has over 400 members and has awarded more than 100 certifications.
Following the continuous efforts on the part of ER doctors, on January 1 of this year the Department of Health (DOH) finally accepted emergency medicine as one of the island's 20 formally recognized specialties and published guidelines for the selection of ER doctors. Shih, who is also the secretary of the SEM, says that before that time many doctors who had seen the American TV show ER wanted to get into emergency medicine but couldn't find a way into the field. Now most local emergency medical specialists first get licensed in another specialty before turning to emergency medicine. Doctors who work in the field from their first year of residency are exceptionally rare.
Huang uses Deng Xiaoping's cat parable, the one which states that whether a cat is black or white doesn't matter so long as it is good at catching mice, to describe the situation in the ER. He says that so long as a doctor wants to be an ER doctor, which field he comes to it from doesn't matter. But an ER doctor's pay is not commensurate with his abilities, something which drives many young people away from the field and means that there is a lack of such doctors in Taiwan.
Dr. Chang Hang, president of the SEM and director of the department of emergency medicine at the Shin Kong Wu Ho-su Memorial Hospital (SKMH), says that in the US, the top five students from any given medical school usually choose to go into emergency medicine. The popularity of emergency medicine in recent years has meant that in addition to being doctors, those wishing to enter the field must also have an M.A. or Ph.D. The main reason for the field's popularity is that ER doctors have set working hours, whereas in most traditional specialties, doctors are always on call. In addition, ER doctors' salaries are second only to those of surgeons. Here in Taiwan, although private hospitals such as CGMH and SKMH have raised salaries, working hours and incomes are still insufficient to compensate for the pressures of the work.
But even though the efforts of many years have resulted in government certification, it is unclear whether the medical community will accept it. Dr. Li Yuan-te, head of internal medicine at NTUH, has trained many outstanding doctors. He thinks that any doctor can work in the emergency room, so it is unnecessary to establish an emergency medicine specialty.
Moving in from the country
"Not having a specialist system for emergency medicine does not have much impact on care at major medical centers. Care in local hospitals spread out all over the island, however, is affected." Chang Hang notes that within the major medical centers, there are many specialties and many doctors. No matter what the time or the specialty, there is someone around. But smaller hospitals don't have the same resources at their disposal. Similarly, large medical centers can have an internist, a surgeon and a pediatrician all on duty at the same time to deal with all those unpredictable conditions that patients come into the ER with. But local hospitals can't necessarily afford the cost of keeping three doctors on duty for a small number of patients.
The quality of care varies at hospitals around Taiwan and this variation is readily apparent in the ER. Although the Guidelines for Treating Emergency Patients stipulate that "Hospitals must immediately examine emergency patients. . . . If unable to provide suitable treatment, the hospital should first take appropriate action, then arrange for the patient to be sent to the appropriate medical institution." But Bullard says that there are gray areas and when faced with a difficult case some small hospitals send the patient on to a major hospital without first stabilizing the patient or contacting an appropriate hospital. Patients whose conditions are too critical to bear this kind of delay often die en route.
From the perspective of "hardware," every hospital has the basic equipment required to monitor heartbeat, blood pressure and body temperature. When a small hospital is faced with a difficult case, all it needs to do is stabilize the patient's vital signs before sending the patient on to a larger hospital. On the hardware side of things, "All you need is some money and there is no problem," says Huang Ying-chieh. An ER's biggest problem is "software," that is, its personnel and its organization.
Many medical centers, including NTUH and CGMH, are already looking for ways to raise the overall quality of medical care and are working with local hospitals to train ER doctors. Many persons are also heading to rural areas to work. Huang Ying-chieh, who worked at the Kaohsiung Medical College (now a regional medical college), is now the director of the Chiayi Christian Hospital. Huang says that although the ERs of the major medical centers are busy, there are plenty of staff. But hospitals at the regional level and below don't have enough staff. He therefore chose to go to the Chiayi-Yunlin area, where the aged make up more than 10% of the population but where the medical care available was not good, in the hope of improving the emergency medical care. He says hopefully, as did Mao Zedong, "We will use the rural areas to surround the cities (and conquer them)."
Private hospitals moving fast
Hospitals are improving at different rates, and private hospitals, where the personnel budget is not as limited as at public hospitals, are taking the lead.
Since 1966, accidental injury has been the third leading cause of death on Taiwan. For those 45 and under, it is the leading cause of death. This circumstance led CGMH to found a trauma center. Dr. Ray Jade Chen, director of the center, says that with the support of CGMH, the trauma center has been given six operating rooms, a 300-bed emergency ward and 22 intensive-care bed-spaces.
Seven years ago, while assistant director of emergency medicine at NTUH, Chang Hang pushed for the hospital to build intensive care rooms for the emergency room. The ER was running out of space and there were emergency patients who could not be admitted to the intensive care units. The hospital, however, would not support him. When he later came to work at SKMH, he got the support of the hospital's administration and SKMH began to train specialists, raised the salary of ER doctors and put into place structures such as ER-related intensive-care units. Four years down the road, SKMH has 10 ER doctors and 25 ER residents. Chang Hang says, "The evidence proves us right. SKMH has implemented these structures well and is causing other hospitals to change the way they run their ERs." But since emergency medicine was recognized as a specialty on January 1, SKMH has lost three attending physicians and three residents to other hospitals.
The triage system
In addition to the strengths of various hospitals, the quality of the whole emergency medical system has been slowly improving under the prompting of the emergency medical community. An example is the triage system which has already been in use in Taiwan's ERs for four or five years. Although it has not been implemented to the same degree everywhere, it is now seen in hospitals of all sizes.
Dr. Liaw Shiumn-jen, director of the primary care department at Linko's CGMH, says that not all patients in the ER need immediate treatment. In North America, ER staff first evaluate the condition of ER patients, using the severity of their condition to categorize them. Those who are in danger, whose life will be threatened if they are not treated immediately, or who must, according to DOH guidelines, be dealt with within two minutes, are category one patients. Category two and category three patients are those that must be taken care of within 10 minutes and 30 minutes, respectively. Category four patients are those who do not have a fever of above 39 degrees C or breathing difficulties or have not been critically poisoned. If these patients can not be persuaded to go through non-emergency channels, the ER may delay their treatment. Shih says that category four patients are often not seriously ill, yet they chase after staff to complain, adding to the difficulties of the ER. Currently, many of those hospitals which have a great number of ER patients have begun to establish evening outpatient services or set up "critical outpatient" services to relieve some of the pressure on the ER.
Another point is that even with the implementation of a triage system, a patient still must rely on the sense of justice and kindness of the person in charge to get in to the doctor. One ER doctor says with feeling, "You just don't realize how many 'untouchables' exist in Taiwan." At some of the major hospitals, a special background, high position or money are pre-requisites for the best treatment. This doctor admits to having received special treatment for being "one of us." He feels helpless in the face of Taiwan's materialistic medical environment. "For people without money, getting a good doctor is a matter of luck."
Fighting for time
This kind of unfair situation is not frequently seen in the ER. With most ER staff involved in life and death situations daily, giving their all to save each and every patient, the most ideal situation would be to be able to extend their feelers out of the ER to the side of every patient in need. Not long ago, pop star Chang Yu-sheng was involved in a serious car accident. When he reached the hospital, he was pronounced dead on arrival. Had there been a trained professional there when he had his accident, he might have been saved.
In any kind of emergency situation, the public usually dials 119, Taiwan's emergency services number. A control center then dispatches an ambulance to take the victim to the hospital responsible for emergency care in that district or to a hospital requested by the victim. The victim, however, may need immediate treatment while in transit or while still at the scene; therefore, emergency medical services must be extended beyond the ER. Taiwan is currently considering a system similar to the prehospital medical care system used in the US wherein trained emergency medical personnel provide prehospital care.
Emergency medical personnel are divided into grades, with paramedics, the highest grade, being required to take 2500 hours of classes before being certified. Unfortunately, as yet there are no paramedics in Taiwan and the burden of most of the prehospital medical care falls on the shoulders of fire department employees. Because fire departments are widely distributed throughout the island, having fire department employees provide prehospital care should be an efficient approach. Unfortunately, although approximately 5000 fire department employees have undergone basic and intermediate emergency medical technician (EMT1 and EMT2) training, few can actually apply their knowledge.
Huang Ying-chieh says with frustration that although the law stipulates that at least two rescue personnel must be present on each rescue mission, a lack of staff often turns an ambulance into a hearse. Naturally, as Chang Hang says, "The ideal situation would be that every citizen knew CPR as well as how to bind wounds, splint limbs and move victims." And this makes the lack of ER doctors that much more apparent. Taiwan needs more qualified emergency medical workers to take on the job of training people.
A new day dawning
Dr. Chan Chi-shean, once the director of Chi Mei Hospital and now the new director general of the DOH, is making great efforts to sort out Taiwan's ERs and has made the improvement of trauma care a major objective. The first stage of his plan aims to improve the problem of ER patients "checking in" to the ER by pushing hospitals to shorten patients' stays in the ER to a maximum of 48 hours and to report how many beds are actually available. In December of last year, the National Health Bureau raised the fees it will pay for emergency examinations by 21% which will encourage hospitals to devote more resources to ERs.
In fact, in August of 1995, guidelines for emergency care passed their third reading in the Legislative Yuan and were put into effect in July of 1996. Among the provisions is one which states that when an "intensive care" ambulance goes out on a rescue or to move a patient, at least one of the persons on its staff must be a doctor, a nurse or an EMT2.
This time the DOH has also rejected its old model wherein it allowed the 19 previously recognized medical specialties to take complete responsibility for certifying their doctors and will itself take on a supervisory role in certifying doctors of emergency medicine. The old method led to problems, an example of which is that of family medicine whose specialists must, like doctors of emergency medicine, have knowledge of all areas of medicine. When family medicine began awarding certifications, many doctors got their certifications but then didn't practice family medicine. For this reason, though emergency medicine has long hoped for recognition as a specialty, it also hopes to avoid handing out licenses too freely, and so is still working on the details with the DOH. Liaw says that if they are not careful, a proliferation of bad doctors will ruin the reputation of the good ones. As for the more than 100 doctors that the SEM has already certified, Chang Hang says that they are all practicing emergency medicine. In the interests of fairness, they may be re-tested, but he emphasizes that, "Overseas, doctors are tested every six years to ensure that they remain sharp."
ER doctors work with lives in the balance. Although their income may not match their output, Chang Kuo-song says that saving one life feels like saving the world. And for emergency patients, making it to the ER is like suddenly getting hold of a piece of driftwood when drowning. With more and more people interested in becoming emergency medicine professionals, maybe the people of Taiwan can begin to hope for a new day to dawn on the island's ERs.
p.106
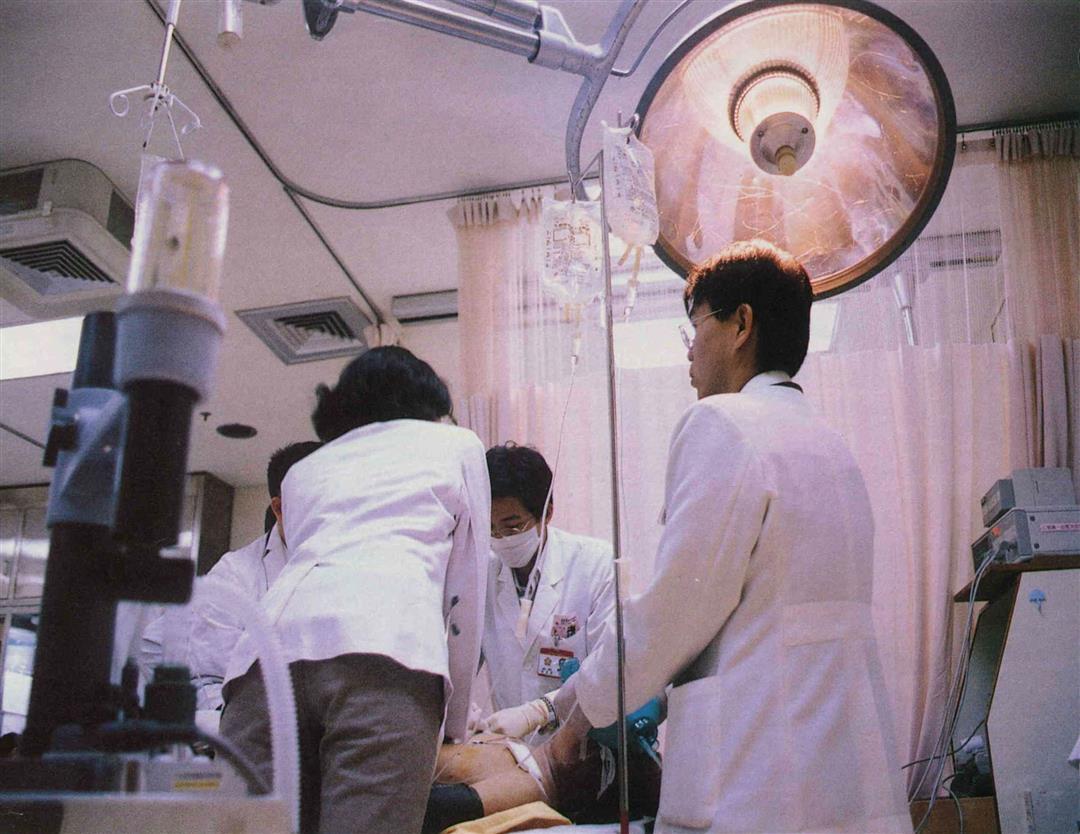
When a patient comes into the ER, teetering on the brink between life and death, the ER doctors rush to him en masse, each taking care of his specific responsibility and doing his best to save a precious life. This is "just another day at the office" in the ER.
p.108
The first stop in the ER is triage. In the ER, patients are not seen on a "first come, first served" basis. Instead they are prioritized based on the seriousness of their condition.
p.109
Ambulances are the vanguard of the emergency room. Unfortunately, ambulances are still a "hit and miss" affair. Some have no emergency care personnel on board, handling the work of rescuing victims with just a driver and a bed.
p.111
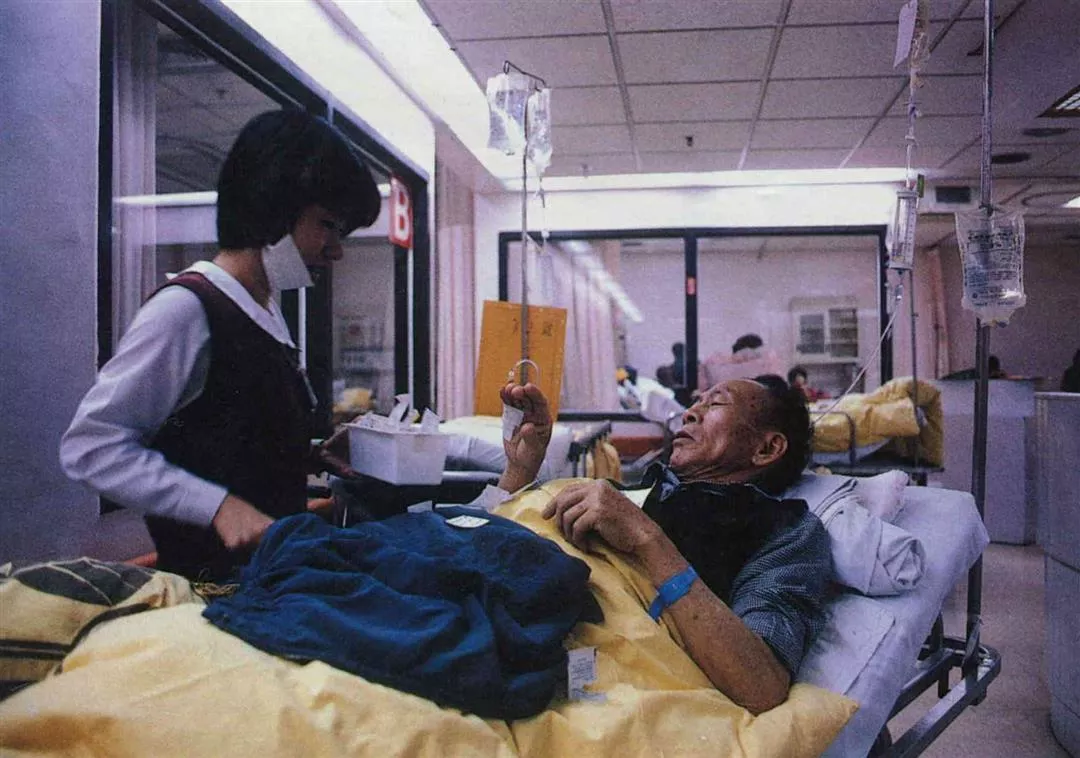
In crowded ERs beds are packed together closely while exhausted family members take turns watching over patients.
p.112
In addition to handling routine emergency medical duties, ER doctors work to further hone their medical skills. In the animal research lab of Taichung's Veterans General Research Building, a group of ER doctors is operating on a small dog as part of advanced training in trauma and life saving treatment.
An ideal emergency medical system would extend beyond the ER, with rescue control centers and local hospitals linked by computer to provide treatment to patients in the shortest possible time.
p.114
Medical personnel and patients both hope that a new dawn will come soon to the island's ERs.

In crowded ERs beds are packed together closely while exhausted family members take turns watching over patients.

In addition to handling routine emergency medical duties, ER doctors work to further hone their medical skills. In the animal research lab of Taichung's Veterans General Research Building, a group of ER doctors is operating on a small dog as part of advanced training in trauma and life saving treatment.

An ideal emergency medical system would extend beyond the ER, with rescue control centers and local hospitals linked by computer to provide treatment to patients in the shortest possible time.
Medical personnel and patients both hope that a new dawn will come soon to the island's ERs.