Never mind those products that the Bureau of National Health Insurance (BNHI) doesn't cover at all and that patients willingly purchase entirely on their own. Let's focus instead on five "balance billing" items, for which the bureau picks up a portion of the cost (see graphic, p. 90). When choosing between these and the more basic options that National Health Insurance fully covers, patients often view the choice as between "something good and something better."
Why only partial coverage?
Sheen Mao-ting, director of the Medical Review and Pharmaceutical Benefits Division of the BNHI, explains that NHI in fact fully covers 90% of the people who need special medical treatments and devices, and that if patients are unsatisfied with its services or have very special needs, then it is not unreasonable for them to pick up a portion of the costs.
Take, for instance, the "rate-responsive"-or "physiologic"-pacemakers that include electrodes and electrical leads for stimulating the heart with a weak electrical current. These can provide for a higher quality of life by allowing patients to increase heart rates while exercising. Nevertheless, ample research shows that they bring no significant drop in mortality rates, so the BNHI has decided that it is "not worth" paying an additional NT$30,000 for these newfangled devices beyond the NT$102,500 it already pays for traditional pacemakers. But out of consideration for those citizens who want the newest and the best, beginning in August 2005 the bureau designated these physiologic pacemakers as "balance billing" items. Patients could elect to pay out of pocket the difference in price between them and traditional pacemakers.
Class divisions in medical care?
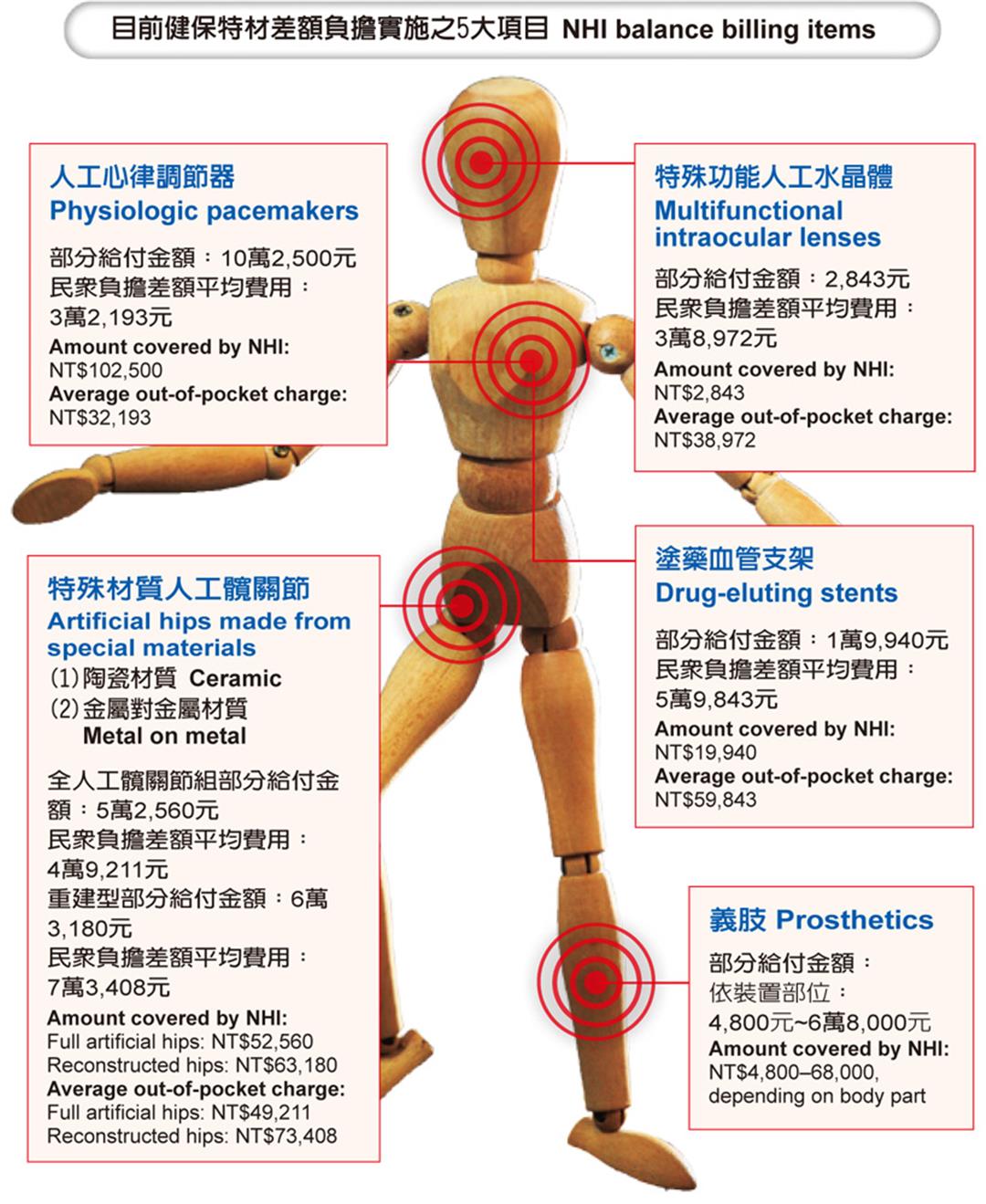
Currently only five items are covered by balance billing: artificial limbs, physiologic pacemakers, drug-eluting stents, artificial hip joints made from special materials, and special-function intraocular lenses (IOLs). For these items, BNHI pays a set amount, and the remainder-ranging from NT$30,000 to NT$70,000-is borne by the individual patient.
Some say that encouraging balance billing will lead to "class stratification" in the provision of medical services, widening the gap in medical care received by the wealthy and the poor. With this in mind, the BNHI decided to stop adding items to the balance billing list in May 2008.
Yet, are the items covered by balance billing really better than those fully covered by NHI? And how many people are willing to pay for these cutting-edge medical products?
Among the five items covered by balance billing, patients have shown the greatest willingness to pay for drug-eluting stents (36%). Physiologic pacemakers (26%) and IOLs (24%) are next, with artificial hips (15%) and artificial limbs (3.82%) less popular. Sheen believes that the disabled, the most likely candidates for artificial limbs, are mostly disadvantaged economically, with little ability to pay a share of the costs.
With regard to the most popular item, drug-eluting stents, one fears that the pros and the cons, including the potential dangers, are not widely understood.
Five years ago, a Mrs. Zhang, who had long suffered from arrhythmia, underwent cardiac catheterization, at which time a balloon angioplasty procedure failed to adequately open her narrowed blood vessels. Right then and there, as Mrs. Zhang lay nervously on the operating table, the doctor suggested implanting stents. At that point drug-eluting stents hadn't been listed for balance billing, so patients would have to foot the entire bill. When her husband and daughters, who had been called into the operating room, heard the doctor say that drug-eluting stents were "better of course" and "longer lasting," they immediately resolved that they wanted the best and were more than willing to pay the NT$100,000 for peace of mind.
Additional functions and dangers
At the end of 2006, drug-eluting stents were placed on the balance billing list. Although that lessened the financial burden, patients were still unclear about how they differed from traditional stents.
Because patients' costs are higher for balance billing items, they tend to want time to consider their options, but doctors, after performing cardiac catheterization, ask patients that have only received local anesthetic to make a choice right on the operating table.
Yet at those moments most patients are in a highly nervous state, and the families also don't have the time to carefully weigh options, so the doctor's recommendation becomes paramount.
Patient decisions are closely connected to doctors' attitudes. Take, for instance, the cardiology department at the private Far Eastern Memorial Hospital. In an average month, about 230-280 surgeries are carried out there, and about a third of these require implanting stents. Drug-eluting stents comprise about half of the total.
"Doctors should give appropriate suggestions to patients," says Li Ai-hsien, director of cardiology at Far Eastern. If patients are too nervous to make a decision, then get them off the operating table and give them some time. When they've reached a decision, another operation can then be scheduled to implant the stents. Li points out that when the situation is critical and there is no time to discuss matters with patients or their families, such as when patients have suffered a heart attack, doctors typically just go ahead and install the kind of traditional stents that NHI covers in order to avoid potential disputes.
The effectiveness of drug-eluting stents is connected to blood-vessel size. Li points out that the decision on the size of stent to use is largely determined by the thickness of the blood vessels needing them. Generally speaking, because short and thick stents (of 4.5 millimeters or greater) are generally installed in the carotid artery, the chance of an issue reoccurring there is low whether or not the stent is drug-eluting. Thinner drug-eluting stents (of 2.25 millimeters) are used with thinner blood vessels to prevent embolisms.
In terms of safety, there is virtually no difference between typical metal stents and drug-eluting stents coated with medicines such as paclitaxel. Li points out that the advantage of drug-eluting stents is that they suppress the multiplication of cells in the blood vessels, reducing by 15% the possibility of an embolism recurring. But that also extends the time to heal. And with drug-eluting stents it is necessary to use platelet inhibitors, such as clopidogrel, for up to a year (metal stents typically require only four weeks of drugs). What's more, in the following year it is necessary to be vigilant to avoid injuries that cause bleeding or surgery; otherwise the patient would have to stop taking clopidogrel (to prevent continual bleeding or hemorrhaging) and the stents would end up actually increasing the risk of heart attacks!
In reality, there is no absolute necessity to implant stents for embolisms. Patients can instead choose surgery or a regimen of drugs. Li points out that research has shown that when a single blood vessel is occluded, there is very little difference in the results between implanting stents and taking only drugs. With numerous blood vessels occluded, there is also no difference in the mortality rates between patients who get stents and those who undergo heart bypass surgery, but those with stents have a higher rate of relapses. But heart bypass surgery is a big undertaking for doctors. In that respect, it's quite unlike stent implantation, which can be completed in just 30 minutes, and which doctors and patients therefore favor.
Solving multiple vision issues
Cataracts frequently afflict the middle-aged and elderly. Every year in Taiwan about 110,000 people undergo cataract surgery. About 80% of these select cataract surgery and intraocular lenses, which are covered by NHI. The remaining 30,000 select more expensive multifunctional intraocular lenses. Implantation of a single multifocal IOL, for instance, requires patients to pay balance billing charges of NT$60,000, and in order to prevent excessive differences between the eyes, two are usually installed together.
Sheen Mao-ting points out that the IOLs that NHI pays for have been in use for 20 years. They're extremely stable and do a good job of restoring vision by replacing the function of the natural lens of the eye that is clouded by a cataract. But without an ability to change focus, they can't simultaneously resolve individual combinations of nearsightedness and farsightedness.
In recent years various new types of intraocular lens have hit the market, including those that are aspherical, multifocal, astigmatism correcting and yellow tinted. Aspherical lenses can increase visual acuity; multifocal lenses can aid vision at near, mid, and long ranges. Yellow-tinted lenses, by filtering out blue light, can reduce the risk of age-related macular degeneration. Patients select from among these lenses based on their particular needs.
When it comes to older people that largely spend their lives in a small area near home, is it truly necessary that they spend a lot of money to return to "ultimate vision"? Opinions differ.
"'What's enough' is the main consideration in determining 'if it's worth it,'" says Tseng Gow-lieng, a ophthalmologist at the Ren'ai Branch of Taipei City Hospital. Overseas, where many old people drive, it's necessary to correct their visual acuity to 0.6 (about 20/35). But in Taiwan, where few elderly drive, then perhaps 0.2 (20/100) is good enough.
Tseng says that after listening to detailed explanations, most elderly patients decide to go with the traditional IOLs covered by NHI. With the additional expense of NT$120,000, economizing seniors tend to feel that the fully covered type is good enough and that it's unnecessary to spend a lot of money to keep up with the latest fashions.
The dearer the better?
Another balance billing item-artificial hips-is also widely adopted by the elderly.
Sheen points out that the femoral stems and heads made out of titanium or cobalt chromium along with acetabular cups made of ultra-high-molecular-weight polyethylene, which are covered by NHI, wear out extremely slowly, typically functioning quite well for 15-20 years. For a patient who is over 70 at installation, the hip should never need replacing.
New ceramic acetabular cups and femoral heads coated in hydroxyapatite ceramic, although having the advantage of wearing out at slower rates, also suffer from the disadvantage of becoming more easily dislocated. And once dislocated, it is likely that more surgery will be required. As for metal-on-metal replacement hips (with both cups and heads made of cobalt chromium), those also wear out at slower rates, and are well suited to the young and those who engage in strenuous exercise. Yet because they release metal ions, which can damage fetuses and kidneys, patients should carefully weigh their pros and cons.
In truth, many newly marketed materials have both advantages and disadvantages. Take, for instance, yellow-tinted intraocular lenses, which block out blue light. Some believe that these can influence mood and prompt depression.
Drug-eluting stents are not miracle devices either. "Drug-eluting stents have their strong and weak points and aren't suitable for every patient," says Li Ai-hsien of Far Eastern Memorial Hospital. Technology is rapidly changing, as are drugs, he argues. The newest drug-eluting stents are not the be all and end all, and patients shouldn't be so "superstitious" about wanting the newest thing.
Because every hospital purchases medical products at different quantities and prices, patients pay out of pocket a wide range of prices via balance billing. Take, for instance, paclitaxel-eluting stents. At Chang Gung Memorial Hospital, they cost NT$43,783, but at the Yangming branch of Taipei City Hospital, they cost NT$65,160. There is a NT$21,000 difference in price between the exact same stent implanted in two different hospitals. For patients who don't shop around, what they pay ends up being a matter of chance.
Unlike handbags, shoes and other consumer goods, choosing between medical products can have a big effect on one's quality of life. Potential pitfalls lie everywhere. Relevant institutions really need to release more data and educate patients so as to keep them from either wasting their money or shortchanging their health.
@List.jpg?w=522&h=410&mode=crop&format=webp&quality=80)






@List.jpg?w=522&h=410&mode=crop&format=webp&quality=80)