Some say that disease prevention is work which, though costly, produces only "invisible" results. Nevertheless, the importance of such work was clearly revealed in the recent enterovirus epidemic.
King Chwan-chuen, a professor in the Institute of Epidemiology at National Taiwan University jests (using a facetious reference to the ROC's former policy toward mainland China) that the attitude of government agencies toward several recent epidemics was "the three no's": no acknowledgment, no response, and striving to convince the public that there was "no need to panic."
The recent enterovirus epidemic (in which many small children died) was no exception. The problem was that the public has lost confidence in government agencies. Given the intensive and sometimes sensational reporting by the media, many parents with small children were frantic, even as government agencies were repeating that there was "no need to panic."
A miracle?
Jurisdiction for Taiwan's epidemic prevention work is shared among the Bureau of Communicable Disease Control (BCDC), the National Quarantine Service (NQS), and the National Institute of Preventive Medicine (NIPM) (all under the Department of Health). The BCDC is in charge of prevention, investigation, research, and handling of incidents of epidemic illness. The NQS is responsible for the collection, exchange, surveying, and reporting of information on epidemic situations internationally. It also assists local public health agencies in some disease prevention tasks. The NIPM is responsible for the manufacture of vaccines, research into disease vectors (the carriers of disease) and pathogens, and inspection work.
Local health public health bureaus also have disease prevention departments. However, the great majority of those working in such departments are not specialists in communicable diseases.
King Chwan-chuen says that Taiwan's epidemic prevention system is in a state of disorder. At the central government level there are "too many cooks," and their division of labor is unclear. When they aren't fighting each other for credit, they're blaming each other for mistakes. Richard Goodman, editor-in-chief of the weekly epidemiology report of the US Centers for Disease Control, has been quoted as saying that, with such confusion among agencies, it is "a miracle" that Taiwan has been able to control epidemic illnesses for so many years.
After the recent outbreak of the fatal enterovirus, the Department of Health (DOH) decided to combine the three central-level agencies into one Bureau for Disease Control, in order to better assign powers and responsibilities. The DOH is also working to amend the regulations governing prevention of communicable diseases. It will list the enterovirus rampant this summer under the second category of the four major categories of communicable illness, which means that hereafter all individual cases must be reported.
The troops on the front line
Fortunately, some communicable diseases can be prevented by immunization. Otherwise the panic over communicable disease would have been replayed in Taiwan even more frequently.
Immunization is the first step in epidemic prevention, and also the most effective method. According to DOH statistics, Taiwan's present immunization rate is 85 percent.
Immunization begins as soon as a baby is born. First come the BCG and the vaccination for hepatitis B. Immunizations continue through first grade, with a series of injections for diphtheria, pertussis, tetanus, polio, measles, mumps, rubella, and Japanese encephalitis. To further reduce the risk of illness, the DOH plans to add hepatitis A, varicella (chickenpox), and hemophilus B vaccinations.
The effectiveness of immunization is easy to see. Take for example hepatitis B, which is widespread among Taiwanese. The DOH began immunizing for hepatitis B in 1985. Over the past decade or so, the "carrier rate" has dropped significantly. According to a DOH survey of six-year-olds about to enter school, the carrier rate for hepatitis B has fallen from the original figure of 10.5 percent to 1.7 percent.
Wu Rong-tsun, director of the Graduate Institute of Biopharmaceutical Science at National Yangming University, feels that there is still a need to upgrade Taiwan's vaccine R&D and manufacturing capabilities. He points out that communicable diseases are regional, and it is necessary to develop one's own vaccines.
Of the vaccines currently received by people in Taiwan, only a small number-such as those for Japanese encephalitis, TB, tetanus, and diphtheria-are manufactured and supplied by the NIPM. The others are all imported from abroad.
Although currently the NIPM is only responsible for developing a second-generation Japanese encephalitis vaccine, its manpower and finances are already stretched to the limit, and it cannot undertake other R&D work. Because the vaccine industry is a high-risk one in which no mistakes are tolerable, few private firms are willing to get involved. Wu Rong-tsun avers that Taiwan should establish a national serology and immunology bureau, and develop its own research personnel.
Fixing the reporting net
Immunization is over 90 percent effective in preventing disease. Unfortunately, vaccines have not been developed for every communicable illness. Shiao Men-fang, director of the Institute of Preventive Medicine at the National Defense Medical Center, says that there are hundreds of communicable diseases, but only a dozen or so effective immunizations.
Wu Rong-tsun says that the main difficulty in manufacturing vaccines is in collecting and culturing the virus. Also, it is not easy to isolate the part of the virus which will produce an immune response.
So how can communicable diseases for which there is no vaccine be resisted?
Wu Tsung-neng, director-general of the NQS, says that for many communicable diseases, the most that can be done at present is to attempt to block their spread. Discovering outbreaks and understanding the overall situation depend on the communicable illness monitoring network.
He notes that at present Taiwan's disease monitoring network includes the legally stipulated case reporting system and local "focal point" communicable illness surveys.
The former is a passive network. It is activated when a doctor anywhere in Taiwan comes across any disease which, according to law, must be reported; the doctor then files a report with the local bureau of public health. The latter network involves cooperation among public health agencies and about 800 doctors nationwide. Each week a telephone survey is done of the situation in various areas, so that there is constant active monitoring of overall public health conditions.
Unfortunately, the recent enterovirus crisis revealed giant gaps in these networks.
Ho Mei-shang, an associate research professor in the Institute of Biomedical Sciences at the Academia Sinica, says that Taiwan's monitoring system only functions for known diseases, but cannot cope with hitherto unknown diseases.
Take the recent enterovirus outbreak. King Chwan-chuen points out that as early as March doctors in southern Taiwan noted a sharp increases in illnesses with symptoms of fever, headache, nausea, and vomiting, and news of a case of death had come out of Chengkung University Hospital by April.
But the epidemic prevention agencies were not alert enough. It was only in mid-May that the NIPM announced: "There has been a increase in cases of illness caused by coxsakieviruses." But government agencies did nothing further, not even conducting laboratory diagnoses.
Another blind spot revealed by the recent crisis is that teaching hospitals are not included in the monitoring network. Yang Yan-shih, a senior specialist at the BCDC, says that the most serious cases were referred to teaching hospitals. Thus the local doctors in the spot check network were not the ones handling the most serious cases, and the government agencies thus overlooked the growing seriousness of the epidemic.
Everybody's an expert
Gaps in the monitoring system were not the only problem. There has also been controversy surrounding the attitude of government agencies.
Early on in the enterovirus crisis, then BCDC director Wang Li-hsin strenuously denied that there was a serious epidemic. He argued that his agency should wait until testing and surveys into the cause of illness had been completed before the agency went public, in order to avoid unnecessary panic and worry.
Sadly, as controversy raged, the epidemic spread, and people were even more panicked and worried because they had no idea what was happening.
Ho Mei-shang suggests that the unwillingness of the government agencies to face the facts even at the height of the epidemic meant that speculation was running rampant, with "everybody acting like an expert" and "people feeling they could say anything." Truth and rumor became confused, creating even more problems for the public.
As King Chwan-chuen concludes, "If the epidemic prevention agencies had simply told people clearly how the disease is transmitted, what steps can be taken to reduce exposure, and what they should do in case of infection, then why would there have been panic?"
Chen Chien-jen, director of the Division of Life Sciences at the National Science Council, notes that the focus of epidemic control is not on the individual, but on determining the geographical spread of an outbreak and on halting its further spread. Thus, measures to slow the spread of the disease should be taken immediately. Using the metaphor of a fire, he says that the first step is to extinguish the flames; there will be plenty of time afterwards to search for the point of origin of the fire and decide what caused it.
Like fire-fighting
It is not always possible to wait to discover the origin of an illness before taking preventive measures. For example, in the US, a tampon was causing toxic shock syndrome in some women. Production was immediately halted, but the cause of illness was only found ten years later. The product was designed to be super-absorbent and long-lasting. But, if the tampon had already absorbed blood, at temperatures of 37* C it became a hotbed for staphylococcus, leading to toxic shock.
In the case of AIDS, preventive measures-especially the use of condoms-were being recommended even while the specific cause was unknown. Condom use was then proven to be effective. Chen Chien-jen therefore emphasizes that if any method of intervention is found, it should be applied immediately.
In the recent enterovirus case, public health scholars were certain that the main channel of transmission of the disease was through fecal and oral transmission. It was rarely transmitted through the air. Thus they instructed people to avoid public places, and to thoroughly wash their hands. Also, swimming pools, kindergartens, nursery schools, and other likely locations for the spread of illness were closed.
"We can't know if this was right or not," admits Wu Tsung-neng. No one knows if the slowing of the epidemic was due to human effort or was a natural trend. However, from the fact that over the same time period other communicable diseases also were reduced, it can be assumed that the preventive measures taken against the enterovirus were effective.
In the trenches
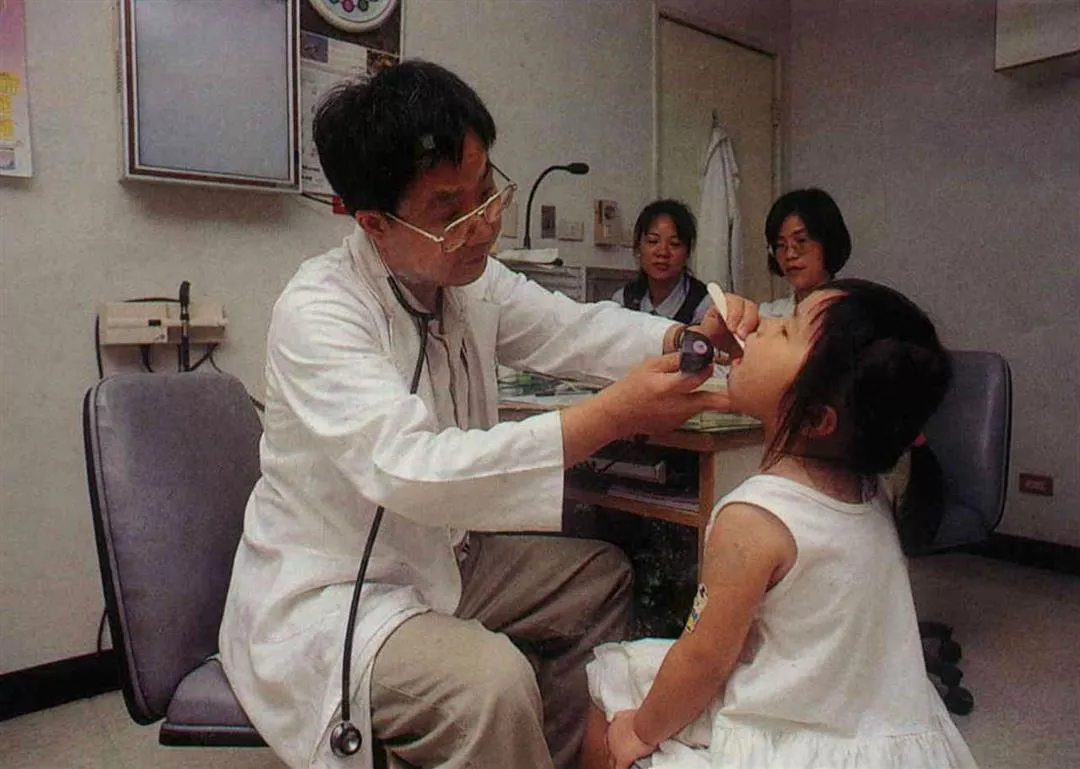
In fact, effective disease prevention still depends mainly on the vigilance of front-line doctors.
This is especially true for those young doctors faced with communicable diseases which have not surfaced for quite a long time. If they are not alert, it is easy to misidentify them.
King Chwan-chuen cites as a case in point the dengue fever epidemic of 1988. Because front-line doctors could not see any clues, when extended treatment failed to make any improvement, cases were turned over to Mackay Memorial hospital. When Mackay diagnosed the illness as dengue fever, it had already been spreading through eastern Pingtung for several months.
In addition, front-line doctors need to have an international perspective. They must have some understanding of the situation in other countries. Chen Chien-jen points out that given the ease and frequency of transportation and the close contacts between people, "an illness 2000 miles away could reach Taiwan in a day."
Besides treating patients, doctors must also have some knowledge of epidemiology. Take for example polio. The rate of occurrence among infected people is from one in 1000 to one in 100. That is to say, when a doctor sees one case of polio, he should immediately recognize that from 100 to 1000 people have been infected, and must on no account waste time by waiting to see what happens.
National defense
Former BCDC director Chang Hung-jen has written that disease prevention is like national defense. Besides preparedness in times of tranquillity, it is necessary to make long-term investments in the weapons needed during "wartime": vaccines, medicines, testing equipment, and serums.
Take for example the crystalbumin used for treating rabies. Although there has not been a case of rabies in Taiwan for nearly 40 years, the BCDC keeps 50 units of crystal-bumin on hand at all time in case of need. Yang Yan-shih points out that the crystalbumin for rabies is extremely expensive, costing NT$30,000 per person. When it reaches its date of expiry, it must be discarded. Each year a significant sum must be spent to purchase it, and this may seem like a waste. However, it is a necessary investment in terms of preventive medicine.
In fact, although disease prevention requires spending money, if it is done right it can save even more money.
Take AIDS for example. Scholars estimate that by the year 2020 the economic losses from AIDS to Thailand will have reached the equivalent of nine years of economic growth.
Yang Yan-shih notes that Thailand and Taiwan recorded their first cases of AIDS at the same time, in 1984. But it was only in 1990 that Thailand began taking preventive measures. Today, the rate of infection among new recruits into the Thai army is 7 percent. In Taiwan on the other hand, blood tests were undertaken early on for soldiers, foreign labor, and those working in "special industries." Currently the carrier rate among servicemen is about 3 in 100,000. Yang argues that the success of Taiwan's AIDS prevention work is due to health education and public awareness campaigns.
Imported communicable diseases
Another important aspect of disease prevention work at present, says Wu Tsung-neng, is blocking diseases from outside from getting into Taiwan. Taiwan, being located in the subtropics, is naturally a hotbed for the spread of communicable illness. In addition, in recent years tourism has developed, travel to mainland China has been allowed, and foreign labor has been brought into Taiwan. As a result of such factors, diseases that had been totally wiped out in Taiwan have come back into the country, creating the possibility of epidemics.
For example, look at this year's dengue fever cases. There were more than 50 as of mid-August of this year, with more than 90% being people who acquired the disease outside of Taiwan. "We have to act fast-faster than mosquitoes can fly," says Wu. If a person infected with dengue fever is bitten by a mosquito before isolation, and the mosquito bites someone else, this could transmit the disease.
The highest period of risk for dengue fever is August and September. Around that time many people travel to Southeast Asia, and may very possibly carry the virus back into the country with them. If there's a typhoon, bringing heavy rains and flooding, leading to a large increase in the populations of vector mosquitoes, the factors of timing, geography, and the human element can combine to create a dengue fever epidemic.
Currently the NQS requires travelers to infected areas to fill out a health declaration upon entering Taiwan. The NQS uses this to monitor the entry of possible cases into the country.
Another focus of Department of Health work in recent years has been tuberculosis. This ancient disease has seen a resurgence of late, causing concern around the world.
New measures to prevent TB include ensuring that patients complete their courses of treatment in order to prevent the rise of drug resistant strains. The DOH has been actively promoting "short-term direct observation treatment." This would compel patients infected with TB to be treated in-hospital.
In addition, in order to close a possible gap resulting from doctors not taking the initiative in reporting illness, and to build a comprehensive epidemiological data bank, two years ago the authorities began using data from the payment of bills through national health insurance for TB medication to find fish that have slipped through the net.
Everyone shares responsibility
Fighting disease is mainly about prevention. But it cannot be denied that prevention has its limits. In particular, once a communicable disease strikes, prevention work is twice as hard and shows only half the results.
Take the case of preventive work to combat the mosquito which carries dengue fever. A survey in Thailand discovered that when people sprayed adult mosquitoes with pesticides, total egg production fell, but the number of offspring which survived actually increased because of the decline of competitors, and the number of disease-carrying mosquitoes ultimately grew.
Teng Hwa-jen, an associate research fellow at the NIPM, notes that a survey of carrier mosquitoes in Chungho by the govern-ment's "dengue fever prevention task force" discovered that, after two years of outdoor spraying of pesticides to kill the insects, the concentration of carrier mosquitoes had returned to its original level.
Thus, besides strengthening the disease prevention monitoring network and increasing the vigilance of local medical care-givers, it is necessary for each person to take a share in disease prevention work, which begins with the individual.
Receiving preventive injections at the appropriate times is a civic duty. Says Chen Chien-jen: "Getting inoculations is disease prevention work that I can do for others and that others can do for me." Only if collective immunity is increased will the possibility of any individual being infected decline.
Obviously, however effective disease prevention work may be, the old saying that an ounce of prevention is worth a pound of cure still apllies.
p.19
Vaccines are the first line of defense. Although they are not 100% effective, if collective immunity is increased, the chances of any one individual getting infected decline. (photo by Chen Pin-chun)
p.20
Modern medicine has reduced the death rate from communicable illnesses, but the concentration of medical treatment and casual use of pharmaceuticals have led to the spread of viruses and the rise of more virulent strains. (photo by Hsueh Chi-kuang)
p.21
Taiwan's environment and culinary customs have combined to make hepatitis B a serious endemic illness. Over the past ten years or so, immunization efforts by public health agencies have led to a significant fall in the carrier rate.
p.22
Studies show that the life cycle of the dengue fever carrier mosquito is affected by temperature. The number of mosquitoes rises with the mercury.
p.23
"Dog bites man" may not be news, but "rabid dog bites man" might be fatal. In recent years, there has been a great deal of contact between Taiwan and mainland China-where rabies is endemic-and public health agencies have to be on guard against the disease "infiltrating" into Taiwan. (photo by Diago Chiu)
p.24
Everyone has a share of responsibility for disease prevention. Cleaning up areas in the neighborhood where disease carriers may breed is one basic way to help out.

Taiwan's environment and culinary customs have combined to make hepatitis B a serious endemic illness. Over the past ten years or so, immunization efforts by public health agencies have led to a significant fall in the carrier rate.
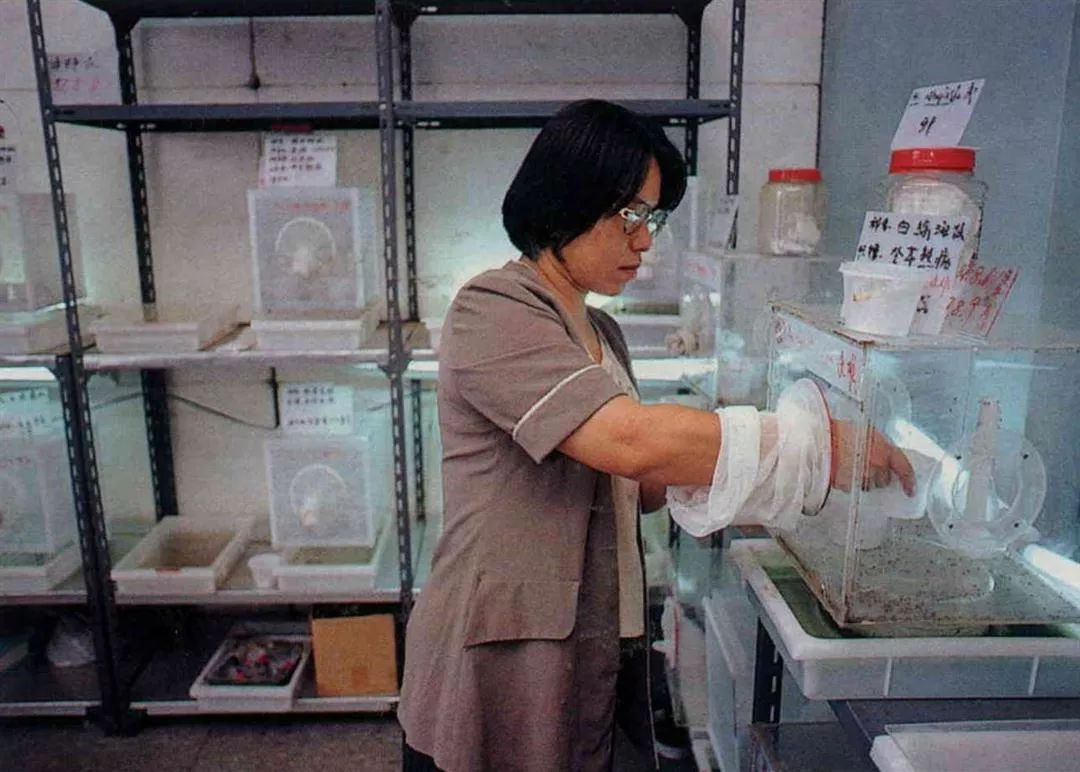
Studies show that the life cycle of the dengue fever carrier mosquito is affected by tempera ture. The number of mosquitoes rises with the mercury.

"Dog bites man" may not be news, but "rabid dog bites man" might be fatal. In recent years, there has been a great deal of contact between Taiwan and mainland China --where rabies is endemic--and public health agencies have to be on guard against the disease "infiltrating" into Taiwan. (photo by Diago Chiu)

Everyone has a share of responsibility for disease prevention. Cleaning up areas in the neighborhood where disease carriers may breed is one basic way to help out.
@List.jpg?w=522&h=410&mode=crop&format=webp&quality=80)






@List.jpg?w=522&h=410&mode=crop&format=webp&quality=80)