At her doctor's suggestion, a woman in the 40th week of pregnancy underwent a Caesarean section. But the nurse-anesthetist mistakenly injected a hemostatic drug (used to control bleeding) instead of the anesthetic, and both mother and baby died.
In another case that hit the headlines, the nerves in a baby's right arm were injured during birth due to a difficult labor with shoulder presentation (incorrect orientation with the baby's arm emerging first). The parents sued the physician for negligence in the prenatal examination. After a trial and appeal, the parties recently reached an out-of-court settlement.
A middle-aged woman went into hospital to have fibroid tumors removed from her uterus. But after the operation complications developed, and she had to have one of her kidneys removed. She took the hospital to court to seek damages.
A plethora of media reports about medical malpractice disputes seem to announce a crisis of confidence between doctors and patients. When patients are dissatisfied with or doubtful about the treatment they receive at hospitals and clinics, the majority choose to remain silent and put their experience down to bad luck, while some voice their concerns directly to the doctor, hospital or local health bureau. But others seek out their elected representatives, complain to the media, throw eggs, carry coffins through the streets in protest, or institute legal proceedings. With disputes between physicians and patients becoming ever more acute, there is an urgent need for fair and just resolutions.
ABC of medical disputes
Legislator Shen Fu-hsiung, who practiced medicine for many years and was a well known kidney specialist, takes a great interest in medical and health insurance matters. He states that a survey of over 30,000 patients in New York State, conducted by Harvard University, found that 3.7% had suffered "adverse outcomes" from their treatment. Of these, 27% could be ascribed to medical negligence. In other words, 1% of all patients had been harmed by medical blunders.
In Taiwan, there has never been an accurate figure placed on deaths caused by medical mistakes, but the number of disputes arising out of medical treatment is considerable.
Ten years ago, a survey conducted for the ROC Department of Health by Dr. Chen Jung-chi, director of neurology at National Taiwan University Hospital, showed that 44% of physicians had been involved in a medical dispute at some time in their career. The four specialisms in which disputes were the most frequent were, in order, surgery, gynecology and obstetrics, orthopedics, and anesthesiology.
Chen Yi-an, a section chief in the Bureau of Medical Affairs at the Department of Health, says that last year the DOH's medical review committee received 406 requests from the courts to provide expert opinions in medical malpractice suits. The committee estimates that only 10% of medical disputes reach the courts. On this basis one can infer that over 4000 medical disputes occur in Taiwan every year.
Cases in which the patient has died account for around 46% of medical malpractice suits. The most common reasons for disputes are adverse reactions that arise in the course of medical treatment, such as postoperative infections, complications, and allergic reactions to medications. The next most common category is dissatisfaction with the treatment process or with treatment outcomes.
Prevention better than cure
"There are quite a number of channels available today for resolving medical disputes, yet neither doctors nor patients are satisfied," says Chen Yi-an. He notes that local health bureaus all have medical dispute resolution units to handle complaints, and hospitals also have similar "treatment concern teams." But generally speaking they are not very effective: doctors and patients each stick to their own versions of events, and in the end cases still go to litigation. This is not only extremely time-consuming, but also very costly both for the parties and for the public purse.
In fact, what many patients are really looking for is not to get compensation or to see doctors punished, but to receive a sincere apology, and for shortcomings to be taken seriously and put right. Liu Mei-chun, an associate professor in National Chengchi University's Graduate Institute of Labor Research, who set up the Taiwan Health Reform Foundation after herself being involved in a medical dispute, is a typical example.
Early in 2000, when Liu was eight months pregnant, she checked into the emergency department of a hospital with abdominal pains. She was there for over two hours before she was seen by a doctor, and the link failed between the fetal heart monitor she was fitted with and the obstetrics nursing station. After several hours, it was found that her baby had no heartbeat, and the doctor later informed her that the placenta had become prematurely detached from her uterus. Thus she lost the child she had been longing for.
"The hospital thought they could solve the problem with money. They didn't respond sincerely to my requests that they should produce plans on how they would improve their administrative procedures and staffing levels in the future. They just went through the motions," says Liu. One mother of a baby with cerebral palsy, who telephoned Liu after hearing what had happened to her, told her: "If back then they had taken my case seriously and the doctor had made improvements, your problem would never have happened!"
Liu Mei-chun filed a criminal prosecution in June 2000, and the case went to trial in May of this year. Although she won the case, Liu was not satisfied with the judgment. The doctor was sentenced to two months' imprisonment, but this was commuted to a fine of just NT$6000, which Liu says has no deterrent or punitive effect whatever.
Mission impossible
"Patients in Taiwan rarely get a chance to have their say." Lawyer Lee Sheng-long, who has been in practice for 27 years and specializes in medical cases, says that court proceedings provide an opportunity to arrive at the truth.
But for most patients, to bring a successful case against a doctor is almost "mission impossible." For instance, in 1991, there were over 2700 medical disputes. 42% were settled by agreement between the parties. Only 10% were settled through litigation, and of these, the patient won in only one case out of ten.
Lee Sheng-long says that in the present environment, the scales are weighted heavily against patients. Patients are unable to obtain their own medical records, and even if they can, the records are not necessarily accurate. The hospital's medical and nursing staff speak with one voice, and whether in terms of physical evidence or witness statements, patients are given no favors. Therefore when faced with cases in which there is no clear evidence of malpractice by a doctor, Lee advises clients not to go any further.
Taking a case to court is also extremely time-consuming, and is grueling both mentally and physically. Lee points out that a case will take at least three or four years to conclude if it goes to a second appeal. If an aggrieved party does not have the determination to see their case through to the end, he will advise them not to embark on litigation.
However, even when patients or their families are determined to go to court, bringing a case is not that simple.
Since the Code of Civil Procedure was amended in 1999, conciliation is compulsory in civil damages cases; only if conciliation fails can a suit be filed. Lee Sheng-long says that this makes the barriers to patients bringing cases against doctors even more formidable. The medical review boards organized by county and city health bureaus around Taiwan are staffed almost entirely by doctors, and the chances of the patient being successful in the conciliation process are practically nil. "In fact, it enables doctors to find out the main points of a patient's complaint, and this gives them a chance to go back and change the case notes," says Lee.
If conciliation fails, the patient can then initiate litigation. But judges still have to rely largely on expert opinions written by doctors. Lee Sheng-long believes that under the current system, expert testimony in malpractice suits also works against patients' interests.
Since the DOH's medical review committee was set up in 1987, it has provided almost all the expert opinions requested by the courts in medical malpractice suits. One-third of the committee's members are laypersons and lawyers, while the rest come from the medical professions. With healthcare professionals accounting for two-thirds of its personnel, suspicions have been raised that the committee is a mechanism for "doctors to protect doctors." In all the opinions the committee has produced since it was set up, it has found the doctor to be at fault in only 20% of cases.
"You can never be sure of the outcome of a court case," says Chen Yi-an. He comments that medical malpractice suits are a great challenge for judges too. Judges without adequate specialist medical knowledge can only rely on expert testimony. Because of this, the Judicial Yuan has proposed reforms to allow experts to assist in judging cases, or to set up specialist medical courts.
Both IQ and EQ needed
In fact, patients are not all bent on embarking on litigation.
According to a handbook entitled Medical Disputes Q&A compiled by the Taiwan Health Reform Foundation, the types of redress most patients and their families wish for are: a reasonable explanation; a sincere apology from the hospital and doctors; financial responsibility to be taken for the continuing medical care of the patient; hospitals and doctors to learn lessons; proposals for specific reform measures; action to prevent similar mistakes happening again; substantive punishment for wrongdoers; reasonable monetary damages or compensation; and only last of all, criminal penalties.
Many of the patients' demands are in fact not hard to achieve. "You can recover from physical injuries, but mental harm is harder to get over." Liu Mei-chun says that when patients sue doctors, they are usually seeking nothing more than justice and a sincere apology.
Physicians themselves are aware that apart from those medical blunders that could and should have been avoided, a large number of medical disputes have their roots in poor communication that results in enormous differences of expectation between doctor and patient about the development of disease.
"It's medical-even if I told you, you wouldn't understand!" "When they think they understand but don't, it's even harder to communicate than when they don't understand!" The impatience of many doctors-perhaps arising from too heavy a workload-also increases the opportunities for medical disputes to occur.
A recent experience of THRF president Chang Li-yun is a case in point.
She had a sore throat, so she went to an ear, nose and throat clinic, where the doctor prescribed some medicine. Chang asked him what the drug was. He replied: "It's something to make you better." She asked again: "Can you tell me what is called?" The doctor said: "It's in English!" "Never mind, please would you tell me!" The doctor replied: "Since you don't trust me, I won't prescribe you the medicine!" Thus Chang left the clinic empty-handed.
"Doctors generally are full of professional arrogance and a self-protecting attitude of blame-shifting," laments Liu Mei-chun.
What's wrong with trying to save people?
However, doctors too face difficulties that outsiders may not understand.
Sherwin B. Nuland, a clinical professor of surgery at Yale University School of Medicine, writes in his book The Wisdom of the Body: "During a long career, I have become accustomed, as have all clinicians, to the necessity of choosing a course of action in spite of unavoidably incomplete information, an as-yet-insufficient state of the supporting science, my own acknowledged subjectivity, and a constantly shifting landscape of medical culture. The urgencies of the bedside demand it." In another passage, he writes: ". . . in some jarringly unforeseen and unwelcome way, the incongruous thought had become more overt in the few seconds it took me to get to the OR: Am I about to botch something up? Will I, in one quick stroke of ineptness and fate, bring my career crashing down around my feet, and with it my sense of what I am? Am I on my way to destroy an unknown patient and myself at the same time?"
Dr. Nuland boldly expresses fears that many doctors secretly share but are afraid to voice.
Gynecologist Lin Wen-pin describes himself as walking a tightrope: "Whenever I encounter an emergency such as acute pain, bleeding, a difficult labor, or a fetus in distress, I have to act immediately. It's as if I were lifting the patient onto my shoulders and carrying her forward onto a tightrope, without a moment's hesitation. . . ."
Dr. Li Yuan-te, superintendent of National Taiwan University Hospital, also observes that while physicians should of course take responsibility for their own mistakes, they are not magicians, and the public should not ask them to take responsibility for matters that are in the hands of God.
One surgeon says that the hostile environment in which surgeons practice medicine causes them to feel that they will be criticized whatever they do, and that they are beset with dangers at every turn. "Other people can be convicted for trying to kill someone, but a doctor can be convicted for trying to save someone!"
To speak from a professional medical standpoint, life is full of uncertainty, and medical treatments are inherently risky. This is particularly true of surgical procedures, and in gynecology and obstetrics. Even with proper risk assessment beforehand, there are great differences between individuals in the degree to which they can stand up to the rigors of various procedures.
For example, "amniotic fluid embolism" is a dangerous obstetric emergency that can occur without any prior warning or symptoms, and may cause the sudden death of a mother during or after labor. Kao Tien-fu, a director of the Association of Obstetrics and Gynecology of the ROC and convener of its medical disputes committee, has encountered two cases, and sadly was unable to save either of the women.
Kao Tien-fu worries that with the burgeoning number of medical disputes, doctors may well seek to protect themselves by adopting a "defensive" approach to treatment, on the one hand carrying out additional, unnecessary examinations, and on the other avoiding risky or difficult procedures. The people who will suffer ultimately are the public at large.
What price life?
To avoid the risk of paying out huge damages claims, American doctors spend an average of 7% of their income on professional liability insurance. But few doctors in Taiwan take out such insurance, mainly because of a general belief among them that taking out high levels of insurance coverage displays a lack of confidence in one's own medical skills. Also, if patients make sky-high claims, whatever insurance doctors have may not be enough.
If life is priceless, by what yardstick should damages for medical negligence be measured?
Kao Tien-fu says that as a result of the China Airlines crash in Japan in 1994, most people have the idea that the life of a Taiwanese is worth NT$10 million. Therefore when patients seek damages in medical disputes today, they generally ask for NT$10 million.
To resolve the growing number of medical disputes, the DOH is considering adopting a "no-fault compensation" system modeled on those in countries such as Denmark, Sweden, Finland and New Zealand.
In May 2000, the Taipei City Health Bureau became the first in Taiwan to introduce a "medical injury compensation system." The bureau appropriated money from the public affairs budget of the city's public hospitals, to set up a fund to provide compensation to patients injured during treatment in city hospitals, regardless of whether the doctor was at fault. There are similar compensation schemes for injuries caused by medications and by immunization.
Compared with the system under the Code of Civil Procedure, which makes conciliation mandatory before a suit can be filed, the DOH's new draft law for handling medical disputes is clearly far more specialized and comprehensive.
Chen Yi-an of the DOH's Bureau of Medical Affairs states that the DOH is planning to train senior judges and lawyers, as well as physicians with at least five years' experience in practice, as medical dispute arbitrators. In future, a doctor and patient involved in a dispute will be able to each nominate an arbitrator, and these two arbitrators will then jointly nominate a third arbitrator, to form a three-member panel to hear the dispute. This will achieve speed, professionalism and confidentiality.
But legislator Shen Fu-hsiung criticizes the DOH's draft legislation, because the decisions of the arbitration panels it envisages will not be binding, and they will not have the power to award damages. He has therefore put forward his own draft of a "Medical Dispute Resolution and Compensation Statute," which separates compensation for medical injuries from the question of fault. In the first stage of handling a dispute, a medical dispute resolution committee will adjudicate the case and award compensation to an injured patient according to a scale of severity. In the second stage, the committee will make a determination as to whether the medical practitioner was at fault, and conduct litigation on the patient's behalf.
Compensation for medical injuries will be paid from a "medical disputes compensation fund," funded half by the general public, and half by medical personnel.
Putting people first
At present, the DOH's and Shen Fu-hsiung's bills to regulate medical disputes are still before the Legislative Yuan, and what the outcome will be cannot yet be predicted. But if the relationship between doctors and patients is to improve, perhaps changing attitudes is even more important than changing the law.
"Courses at medical schools lack humanistic content, and they fail to give training in communication. The result of putting too much emphasis on specialist knowledge is to create an attitude in doctors of not treating patients as people. This is something we should work hard to correct," says Chen Yi-an.
"The doctor-patient relationship is crucial." Kao Tien-fu agrees that although doctors need to be specialists, they also need to understand and empathize with patients' feelings. With a better doctor-patient relationship, many medical disputes could be easily resolved.
"Putting the patient's interests first is doctors' prime duty, but in return patients should also trust doctors." The director of surgery at one medical center, who did not wish to be named, states that surgeons are exposed to long-term stress, and their life expectancy is ten years less than the average. For example, he himself goes to the hospital at 6:30 every morning, and does not return home until nine at night. But however tired or busy he may be, he never lets the phone ring more than three times before answering it.
He says with feeling: "Resolving medical disputes is a post-hoc approach. If you want to prevent disputes before they happen, the solution is to rebuild medical ethics and improve the doctor-patient relationship."
Undeniably, medical science has its limits. The fight against disease is full of risks, and this is something that both doctors and patients need to recognize and accept. If doctors hold fast to their prime duty of saving lives and putting the patient's interests first, and treat patients with sincerity, then surely medical disputes need no longer be an unbearable burden for both doctors and patients. l
p.028
It takes a professional and caring attitude on the part of doctors to overcome patients' feelings of helplessness and the fears of their family members. Communication and mutual trust are the basis of the doctor-patient relationship.
p.030
(facing page) Any surgical procedure entails risks for both doctor and patient. The medical team's careful and unstinting efforts are the best guarantee of success.
p.031
Doctors work from early till late amid the smell of medicaments and the groans of suffering patients. As they make their morning rounds, it is only their sympathy for patients that gives them the courage to carry on.
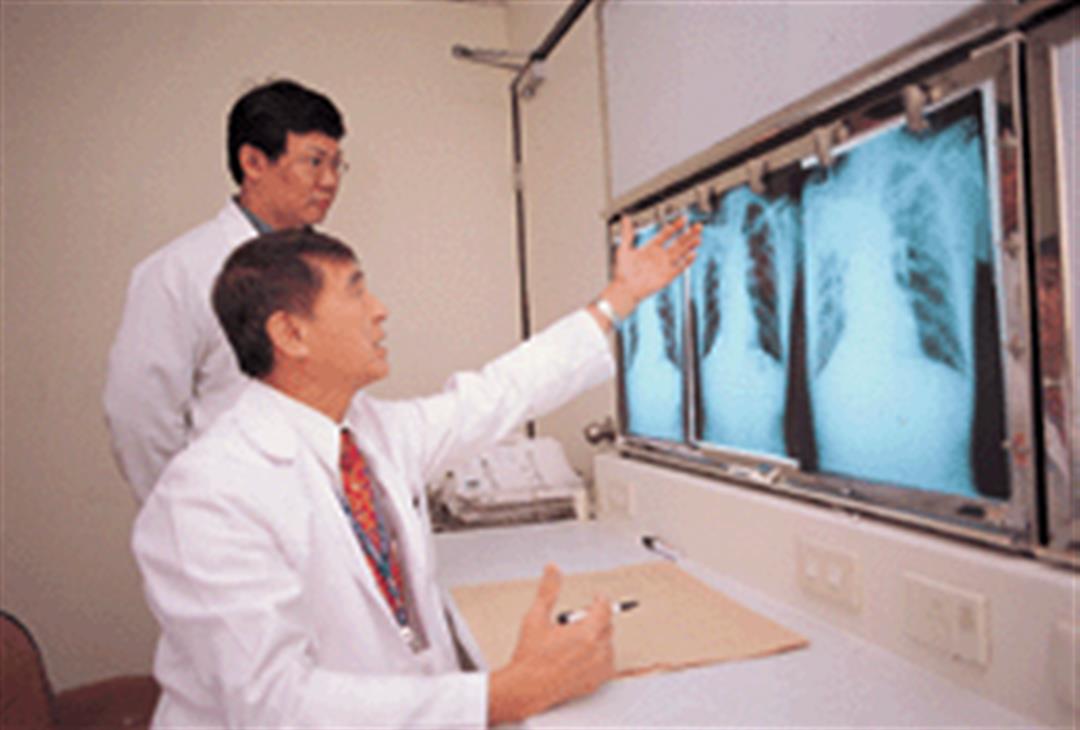
p.033
Ascertaining the patient's condition is the first step toward diagnosis and treatment. When faced with a serious disease, doctors are sure to proceed cautiously and discuss the case with colleagues.
p.033
A doctor's friendly and patient attitude is like a breath of spring for patients, and makes their ailments easier to bear.
p.034
If doctors approach patients and their families with a caring attitude, appreciate their suffering and empathize with their feelings, the doctor-patient relationship is sure to be a harmonious one.











@List.jpg?w=522&h=410&mode=crop&format=webp&quality=80)