On August 9, 1988, a large group of journalists gathered in the Tri-Service General Hospital in Taipei. When heart recipient Yi Pien, with a nervous smile on her face and accompanied by the Director of Cardio-vascular Surgery at the hospital, Wei Jeng, entered the patient discharge room, the crowd exploded in applause. After four consecutive deaths of heart transplant recipients, this fifth recipient was walking out of the hospital glowing with vigor.
On July 17, 1987, Chu Shu-hsun, Professor of Surgery at National Taiwan University Hospital, performed an emergency heart transplant on a patient, marking the first successful such operation in Southeast Asia. This set off a flurry of activity in the R.O.C. and within a month three more such surgeries were done, and debates broke out over brain death, organ donation, experimental surgery with humans, and inter-hospital competition.
Alas, this was but a passing flurry. Only one of the four patients survived rejection and infection to leave the hospital, and he later died from failure to continue taking his medication. These disappointments, plus the decision by the Department of Health to classify heart transplants as "human experimentation" (so that the costs of the operations are to be taken up by the hospitals), caused heart transplants to quickly fall into a period of assessment of previous experience.
Dr. Cheng Kuok-kei, Director of Cardiovascular Surgery at Veterans General Hospital, and the main surgeon in the second and sixth transplants, points out that "using as a standard that in the U.S. and Europe surgery is successful 100 percent of the time, that 85 percent of the patients live beyond one year and 70 percent beyond five, the performance in the R.O.C. has not been brilliant. But this does not mean the quality of medicine in the R.O.C. is lower."
Dr. Wei Jeng has a similar view, noting that "the techniques of heart transplant surgery are not difficult; the problem is in correctly gauging and selecting a suitable patient, and in post-surgery medication and rehabilitation. There is no formula to follow, and one cannot have excessive hopes that the operation, once decided, will be a success."
The experience of the U.S. and Europe gives encouragement to the R.O.C. medical world. Dr. Chu, despite having lost the battle for three patients, affirms that "heart transplants will become one of the main methods for curing heart disease; we must develop heart transplantation domestically not for glory or to please the public, but because it is an objective need."
Heart disease is the number four killer in the R.O.C., taking nearly ten thousand lives a year. Although the quality of open-heart surgery in the R.O.C. is second to none in Southeast Asia, and most patients can be helped through surgery, there are still some for whom surgery is not enough. The number of patients whose illnesses require heart transplants is close to one hundred per year.
The deaths of the first four recipients was of course a major reason why patients have been unwilling to undergo heart transplants, preferring to face death than face the problems of the surgery. This passive attitude has been a severe disappointment to doctors eager to stay active.
As for the new start made with Yi Pien, for example, she is illiterate and had never even heard of heart transplants before heart failure forced her into the hospital. Her daughter, Yang Miao-ling, in order to reduce the psychological pressure, simply told her, "Your heart doesn't work any more, It is best to change to a healthy one." After a year of severe illness, Yi finally concluded, "If the doctor says I can't go on without a transplant, then do the transplant!"
Yi Pien's acceptance of her fate and the fact that her family did not have excessive expectations eased the psychological burden of Dr. Wei, the surgeon, who proceeded to smoothly complete his first transplant. Drs. Chu and Cheng happily wish Yi continued health, hoping that success in her case will put heart transplants back on track and help raise medical standards in the R.O.C.
Besides confidence problems, patients in the R.O.C. also have a tendency to wait until the last minute before opting for surgery. As opposed to the U.S., where transplant patients have a six-month waiting period to prepare physically and psychologically, patients in the R.O.C. put off surgery until their case has reached a near-fatal stage. Recent recipient Ts'ai Yu Jui-chu, for example, had been in and out of the hospital four times for heart problems and was failing fast before deciding on the surgery, making it tougher for doctors to achieve a complete return to full health after the transplant.
Even if a patient is willing, however, this does not mean he/she is suitable. With the lessons of the first four failed transplants in mind, much emphasis has since been placed on pre-surgery selection. Dr. Cheng lists three "absolute conditions," which are to have absolutely no infection, no trace of cancer, and healthy lungs. The first two conditions are necessary because, to lower the chances of rejection, the patient's immune system must be deliberately weakened; infections or cancers could then quickly spread. The third is necessary because a weakened heart increases the chances of irreversible pulmonary hypertension, which causes the lungs to fill with water.
Dr. Cheng also has "relative conditions" too numerous to mention, including factors of age, drug or alcohol dependence, and spiritual stability.
Thus a heart transplant takes much more than a good surgeon: it takes skill in bedside manner, in psychology, in immunology and a variety of other medical specialties, and even social work. It takes a degree of care much beyond that of other organ transplants to enable the patient to survive.
As for the surgery itself, it is not especially difficult; "about the same as open heart surgery" according to Dr. Wei. But the surgery is only a start. Postsurgery care is crucial.
The most immediate problem is "rejection." Dr. Chu often uses a vivid analogy to explain this phenomenon: "Everyone has some resistance capacity; when an unknown object enters the system, the immune system is alerted and rejects and destroys the object. Its function is much like that of national defense, except that a national defense can tell whether an intruder is friendly or hostile, while the body's immune system cannot tell 'friend or foe' and has no mercy on the transplanted organs."
To keep watch on a possible rejection, the patient must go every week in the first month or two for the taking of a small piece from the heart by way of an inserted tube. While uncomfortable, this is thus far the most reliable method for investigating the condition of the new heart.
The invention of the medicine cyclosporin in 1980 has helped brighten the prospects for resisting rejection. But, as noted, it works by weakening the immune system, making even an ordinary cold "fatal" to the transplant recipient, in Dr. Cheng's words.
Selecting the dosage is thus crucial, and the optimal balance between resisting rejection and resisting infection is widely debated. Even still, points out Dr. Wei, for some patients there is no optimal balance and they succumb to one or the other.
Besides weakening immunity, moreover, the commonly used drugs cyclosporin, speroid, and imuran have further side effects, including possibly inducing kidney failure, raising blood pressure, and more. Cyclosporin may cause a type of cancer similar in effect to AIDS, while speroid may increase the desire for food. Because it is necessary to take these medications for one's entire life, they are used in combination to minimize the dosage and the side effects.
The post-surgery spiritual condition of the patient also requires extreme care. In Ts'ai Yu Jui-chu's case, despite prior discussion with her doctor about what to expect, within a week she became anxious, depressed, and pessimistic. Further, if the patient is dissatisfied with the speed of recovery, he/she may wonder if the heart of the donor is "playing tricks" or if the doctor had not deceived him/her in some way. If the patient can make it the first month in good physical and psychological condition, then the chances of full recovery are greatly enhanced.
And after going home? Says Dr. Wei confidently, "A heart transplant recipient can absolutely enjoy a healthy and happy life."
[Picture]
A Table of Heart Transplant Recipients in the R.O.C.
[Picture Caption]
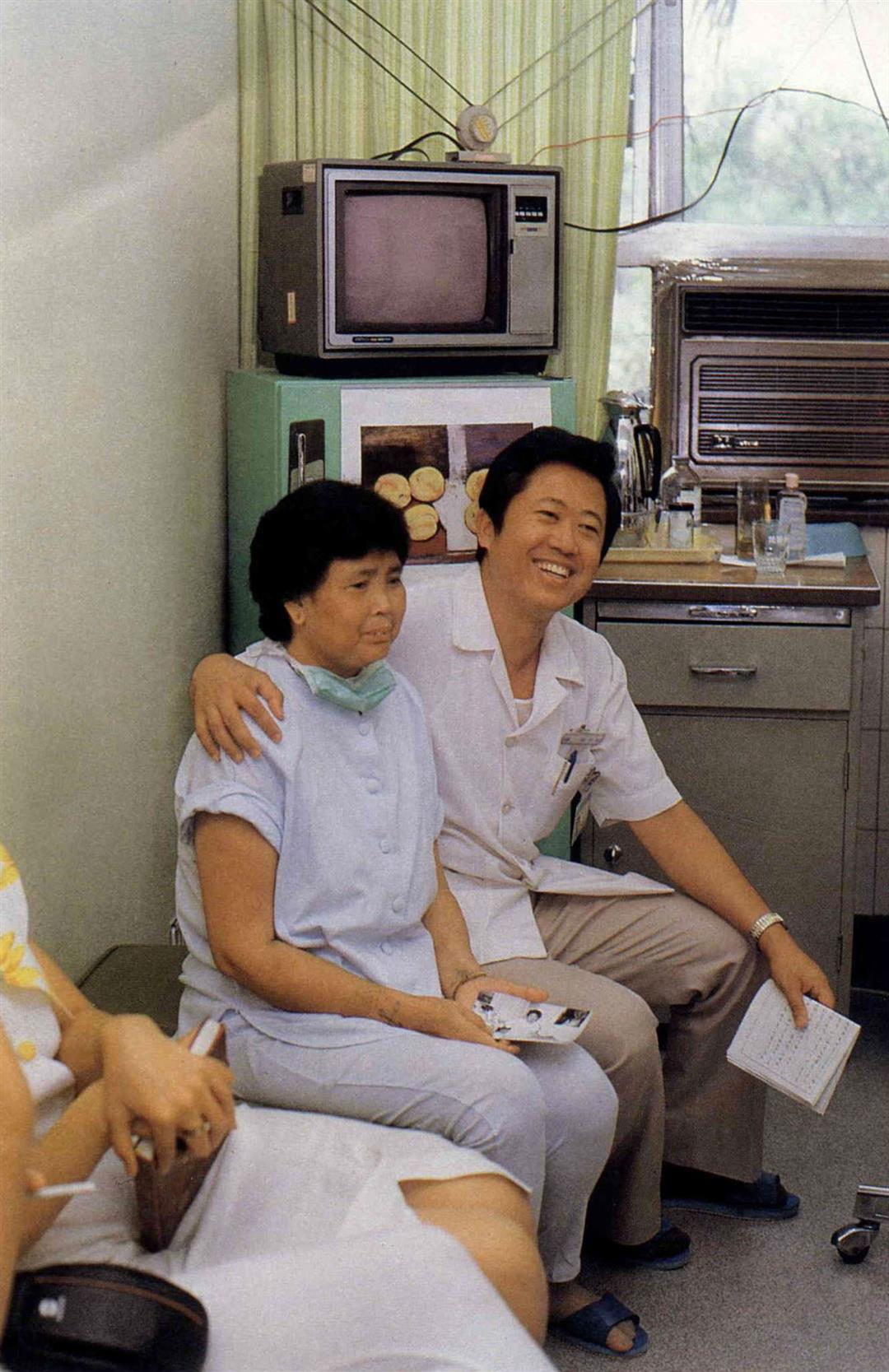
At her "coming out" press conference, Yi Pien cried and smiled. Seated on the side is Dr. Wei Jeng, standing in back are daughter Yang Miao-ling and hospital staff.
When Yi Pien walked out the door of the Tri-Service General Hospital, she was met by a host of reporters and by the hopes and good wishes of everyone.
Yi Pien and Wei Jeng developed mutual trust and a close friendship over the course of their common struggle.
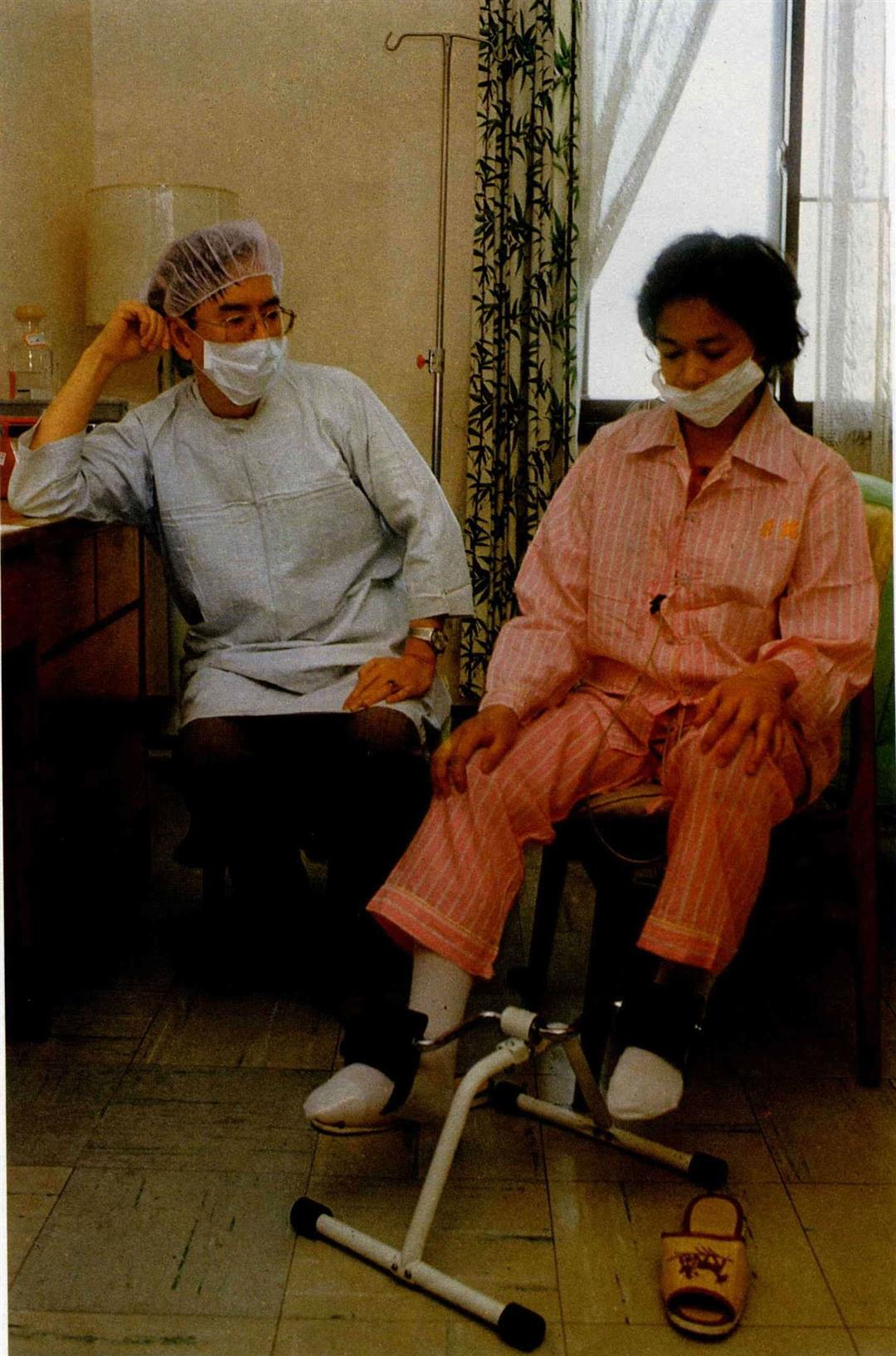
Doing rehabilitative exercise is crucial for the recovering transplant recipient; the photo shows recipient Ts'ai Yu Jui-chu and Dr. Cheng Kuok-kei of Veterans General Hospital.
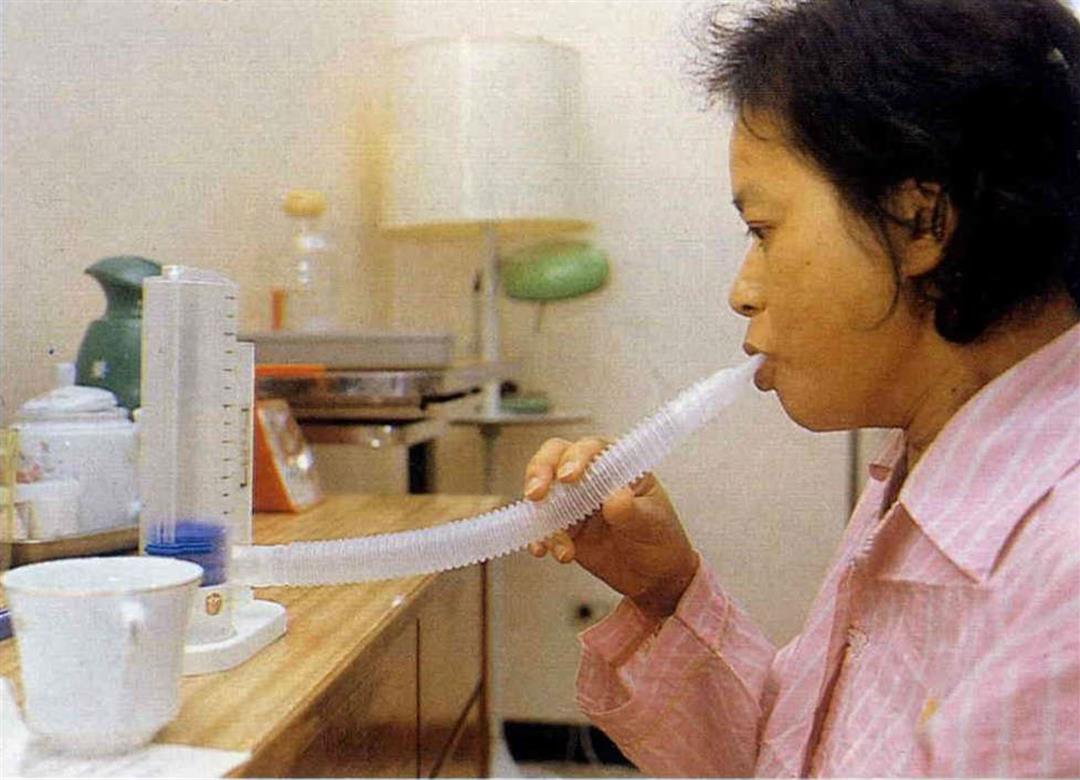
"Inhale deeply, exhale slowly" to train the function of the lungs. This too is part of rehabilitation.
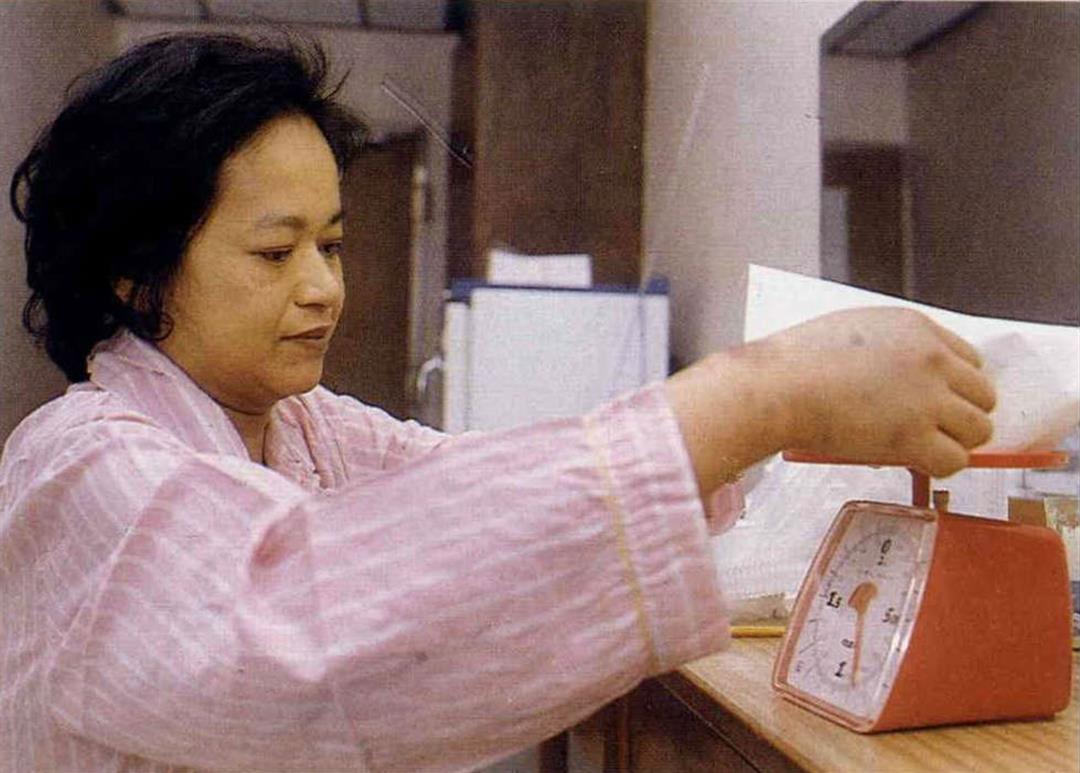
In order to prevent patients from gaining too much weight from the increased appetite that comes as a side effect of the medication, meals are carefully measured and recorded.
The conflicting demands between preventing rejection of the new heart and fighting infection pose a potentially fatal dilemma, illustrated here in a cartoon by Chu Shu-hsun.
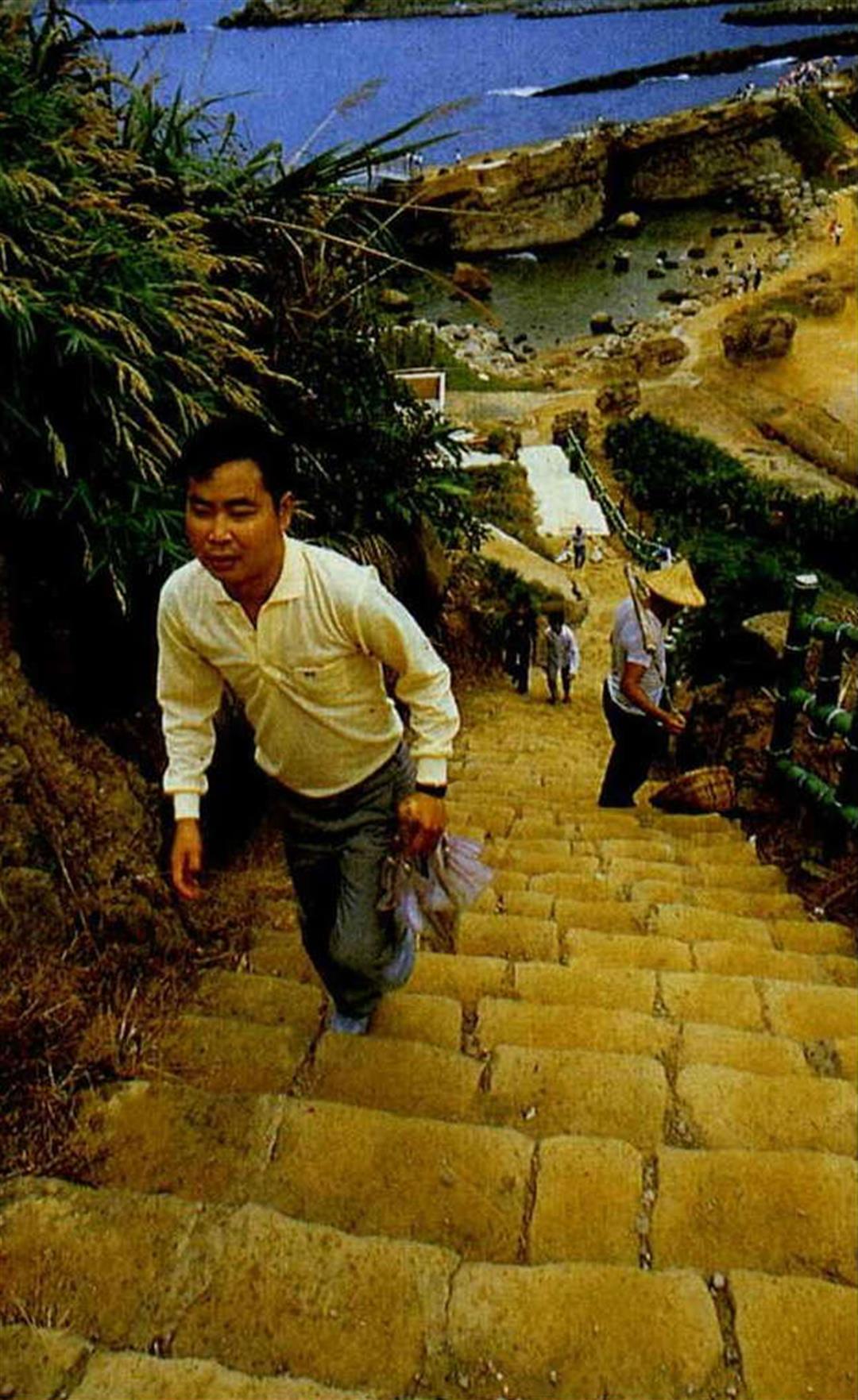
When recipient Sung Kuo-shan left the hospital, he was in good enough shape to climb the steps at Yehliu without breathing hard. Unfortunately, his failure to continue taking his medication undid all the hard work of surgery. (photo by Chang Chia-jung)
At home amidst her children and grandchildren, Yi Pien affirms that "Life once again has value."

When Yi Pien walked out the door of the Tri-Service General Hospital, she was met by a host of reporters and by the hopes and good wishes of everyone.
Yi Pien and Wei Jeng developed mutual trust and a close friendship over the course of their common struggle.
Doing rehabilitative exercise is crucial for the recovering transplant recipient; the photo shows recipient Ts'ai Yu Jui-chu and Dr. Cheng Kuok-kei of Veterans General Hospital.
"Inhale deeply, exhale slowly" to train the function of the lungs. This too is part of rehabilitation.
In order to prevent patients from gaining too much weight from the increased appetite that comes as a side effect of the medication, meals are carefully measured and recorded.

The conflicting demands between preventing rejection of the new heart and fighting infection pose a potentially fatal dilemma, illustrated here in a cartoon by Chu Shu-hsun.
When recipient Sung Kuo-shan left the hospital, he was in good enough shape to climb the steps at Yehliu without breathing hard. Unfortunately, his failure to continue taking his medication undid all the hard work of surgery. (photo by Chang Chia-jung)

At home amidst her children and grandchildren, Yi Pien affirms that "Life once again has value.".


@List.jpg?w=522&h=410&mode=crop&format=webp&quality=80)
@List.jpg?w=522&h=410&mode=crop&format=webp&quality=80)




@List.jpg?w=522&h=410&mode=crop&format=webp&quality=80)