Early discovery, early treatment?
Why has tuberculosis been so difficult to eliminate?
For any disease, early detection and early treatment are the most effective control measures. But for TB, achieving a correct diagnosis early in the course of the disease and a subsequent complete treatment regimen both present challenges.
Discovered a hundred years ago, the Bacillus Calmette-Guerin (BCG) vaccine is still used to prevent TB. In Taiwan, excepting infants with genetic diseases or those born prematurely, 98% of newborns are given a BCG vaccination in order to prevent tubercular meningitis.
However, the vaccine remains effective for only ten years, and provides no immunity in adults. In other words, once past the period during which the BCG vaccine can provide protection, everyone runs the risk of infection and of contracting TB.
Interestingly, statistics reveal that tuberculosis afflicts males and females unequally, with males three times more likely to contract the disease. Suo Jen, a tuberculosis specialist at Taoyuan General Hospital, points out that before the age of 35, the disparity between males and females is not great. But with advancing age, the difference becomes increasingly evident, and by age 67, the ratio of male to female victims reaches three to one. Some surmise that the disparity is related to hormonal effects, but as yet no firm conclusions have been reached.
Furthermore, due to factors such as the presence of other chronic illnesses and weakened overall resistance to disease, the elderly are the group with the highest incidence of TB. Currently, of the 19,000 reported suspected cases of tuberculosis in Taiwan, 46% are among persons aged 65 or older.
More unusually, Taiwanese Aborigines are also a high-risk group for tuberculosis. Though they are home to only 1% of Taiwan's total population, the mountain villages largely inhabited by Aborigines account for 3 to 5% of all reported cases of TB. According to statistics, the incidence of tuberculosis in mountain villages is four times higher than in the plains, while the mortality rate is six times greater. Suo believes that the high incidence and mortality of TB in mountain villages may be related to such factors as Aborigines' economic status, education, environment, lifestyles, personal hygiene, and willingness to seek and comply with medical advice.
Although TB is an ancient disease, the factors influencing its pathological course remain unknown. In other words, it is still a mystery why some people develop active cases after infection, while others do not. However, when a person is infected by the TB bacillus, he will not usually immediately develop full-blown tuberculosis, and the bacterium may remain latent inside the body for a long period of time. Generally speaking, once infected, there is a roughly 10% chance of a person developing an active case during the rest of his life. Of those who do develop TB, half do so within five years of infection. Once the full-blown disease emerges, if the condition goes untreated, one out of two people will die within five years. Another quarter of such patients will see their TB go into remission, a state where it is no longer active, though it may reemerge at any time. In addition, in one out of four patients, the disease becomes chronic and the person may continue to infect other people.
As far as we know, of those persons who are in close contact with an infectious tuberculosis patient-such as family members and co-workers-roughly one in three will become infected. A patient with an active case of tuberculosis can on average infect ten to 15 healthy people per year with the TB bacillus.
Due to the long latency period, early detection of TB is very difficult. And even if a patient already exhibits some minor signs of the disease, a correct diagnosis is also not easy.
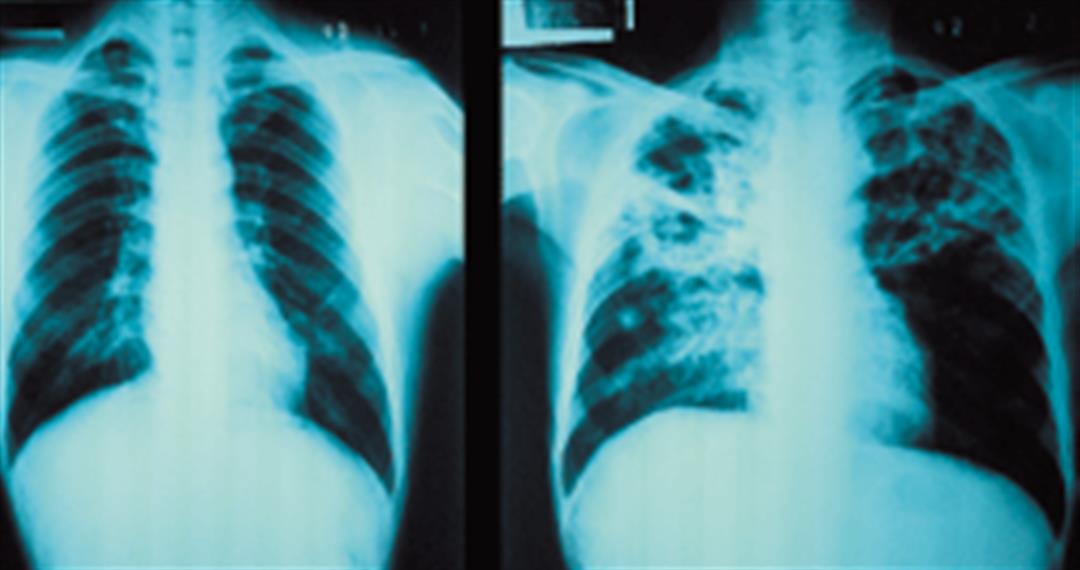
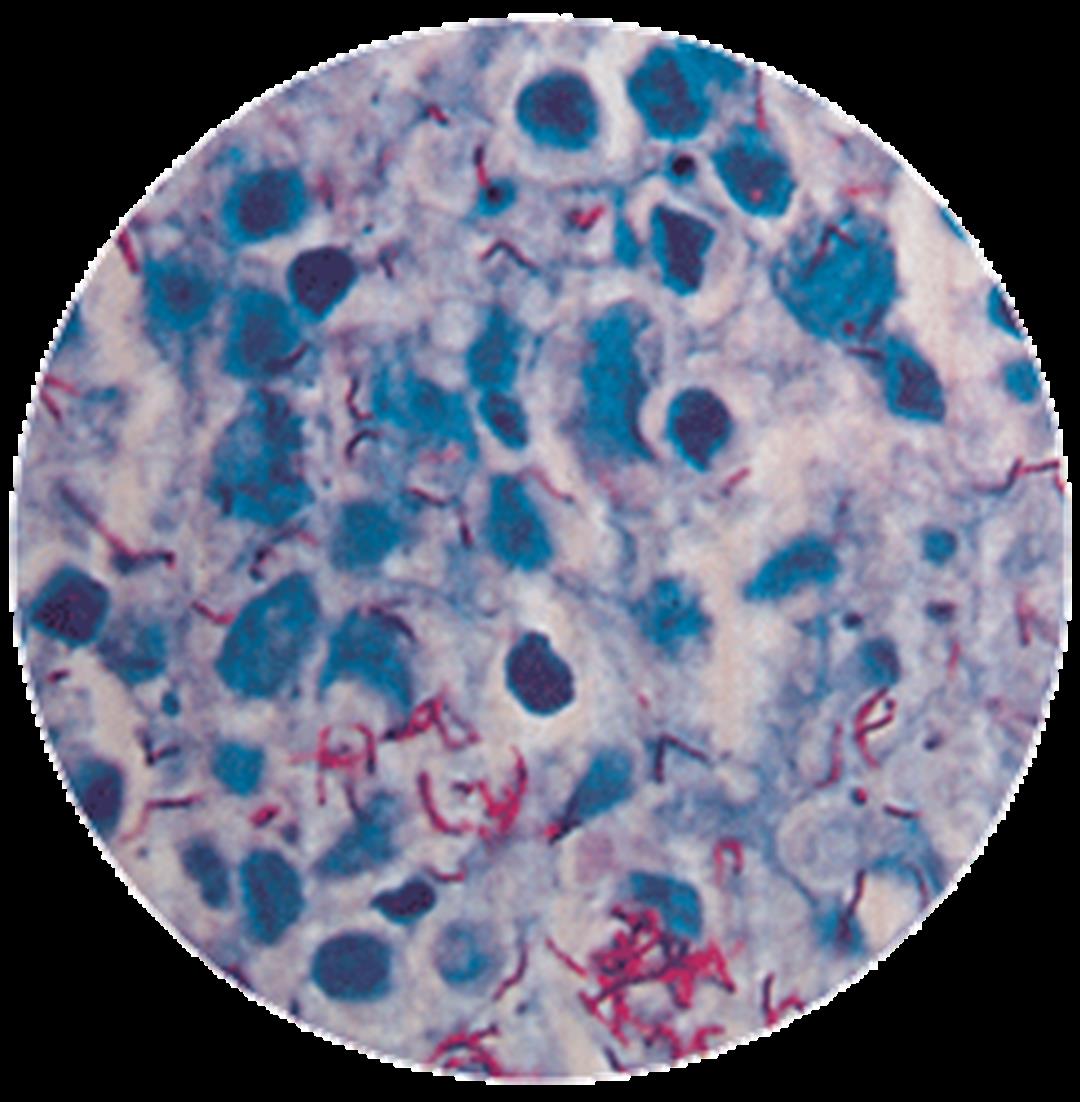
A chest X-ray and sputum tests are the current methods for establishing a tuberculosis diagnosis. However, these two methods both have their blind spots. Chest X-rays will not necessarily be able to accurately capture lesions, as the lungs have five lobes, and there are more than 100 different types of bacillus that commonly infect the lungs. Moreover, tests of sputum will not always reliably detect M. tuberculosis. Under these circumstances, a physician's experience and professional training are extremely important.
Statistics show that two or three months typically elapse between the time a TB victim first shows symptoms and when he seeks medical assistance. Then from that time until a diagnosis is confirmed and treatment begins, another two or three months usually pass. In other words, from the time a tuberculosis victim first shows symptoms of the disease and the time when treatment begins, an average of half of year will have gone by. This lengthy period provides a window of opportunity for further infection that is very difficult to control.
After discovering tuberculosis, comprehensive treatment is yet another challenge.
Tuberculosis is not an untreatable illness. Generally speaking, if only medication is taken properly for two weeks, the patient will no longer be infectious, and continuing this course for six to nine months will effect a cure.
Patients with active tuberculosis must be quarantined and given treatment in a hospital until the infectious period is over. At present, there is only one hospital specializing in tuberculosis in all of Taiwan-Taipei's Hospital for Chronic Diseases, which maintains 17 negative-pressure isolation rooms used specifically for patients with active TB.
After the first phase of treatment is completed, and it has been confirmed that the patient's sputum is pathogen-free, the patient can be allowed to leave the hospital. After being discharged, patients must continue to take medication for six to nine months. Because they must swallow six or seven pills every day over a long period-with some patients developing side effects such as liver damage and loss of appetite-patients often cannot tolerate the drug treatment and quit before completing the full course of medication.
If treatment cannot be completed, it will result in a very serious consequence-the creation of drug-resistant bacterial strains, which are a thorny problem for current efforts to control pulmonary tuberculosis. Joz Lu, director of Taipei's Hospital for Chronic Diseases, points out that once the M. tuberculosis in a patient's body develops drug resistance, his tuberculosis becomes both chronic and active. Not only will such a patient's own illness be extremely difficult to treat, but if the drug-resistant bacterial strain harbored by the patient's body infects other people, they too will become carriers and victims of the same intractable form of tuberculosis.
Tuberculosis prevention postage stamps issued by the National Tuberculosis Association. Such stamps were used both to raise funds for tuberculosis prevention efforts and to raise public awareness. (courtesy of the National Tuberculosis Association)








@List.jpg?w=522&h=410&mode=crop&format=webp&quality=80)
@List.jpg?w=522&h=410&mode=crop&format=webp&quality=80)




