The debate centers on questions of what exactly National Health Insurance should be. Is it insurance or is it welfare? Is fairness more important or efficiency? While there may be no right or wrong answers to these questions, how they are ultimately addressed will affect the future direction of the National Health Insurance system and the welfare of all the residents of Taiwan.
When the National Health Insurance Law was being reviewed by the Legislative Yuan three years ago, legislators were unable to reach a consensus on issues including whether the system should be public or private and how it would be paid for. In the end, in order to get the system up and running on schedule, the legislators tacked two so-called "sunset clauses" onto the bill and passed it. These provisions, articles 85 and 89 of the National Health Insurance Law, state that within two years of the institution of the National Health Insurance system, the government body responsible for overseeing the system must propose comprehensive reforms to its funding, its organization and to the financial responsibilities of those insured under it. In addition, the law states that within two-and-a-half years of the system's implementation, the Executive Yuan must revise the National Health Insurance Law.
Rescuing National Health Insurance
In accordance with these articles, in July of last year, the Department of Health (DOH) made proposals to reform the system. The DOH recommended changing the system from one which is publicly established and publicly run into one which is publicly established but privately run. In February of this year, the DOH revised its proposal, suggesting that the nation's health insurance market could be thrown open to competition between two or three private insurance companies.
When the proposals were sent to the Legislative Yuan for review, they immediately caused a stir which rivaled that which took place when NHI was first implemented. Everyone had an opinion.
Supporters of the measures included Hsin Ping-lung and Hsueh Li-min, researchers at the Chung Hua Institution for Economic Research, and Huang Weng-hung and Chen Hsiao-ping, welfare scholars. They believe that having a government-run system is inefficient and that privatization and competition are the trends of the day.
But many are opposed to the reforms. Lin Wan-i, chairman of the Department of Sociology at National Taiwan Univeristy, drew together more than 300 groups representing laborers, the handicapped and women into the "Alliance to Rescue National Health Insurance," dedicated to opposing the privatization of NHI. Lin believes that under the guise of fostering competition, the government will, in fact, be granting a monopoly which will result in "insurance by the corporations, not for the people."
Hospitals and clinics which provide basic medical care also responded strongly, stating that they would rather be the servants of the nation than the slaves of the corporations.
Those insured by NHI, however, are uncertain about how they should respond. Instead, they seem to be persuaded by the logic of whomever happens to be speaking at the moment. They don't know which side to support and in general seem confused about why the government would want to change an NHI system which they feel is working.
96% participation
NHI, which left many key issues unresolved when it was implemented in March of 1995, satisfied only 20-30% of the public in its initial phase. However, as the public has begun to use the system and come to understand it better, their satisfaction with it has risen. Surveys taken by the United Daily News, the Min Sheng Pao, and the Chinese Institute of Public Opinion in fiscal 1998 indicated that more than 70% of the public were satisfied with NHI. And in a survey taken early this May, more than 75% of the public were satisfied with NHI.
Over a period of more than three years, the government-established and government-run NHI system has demonstrated valuable capabilities and earned high marks.
One praiseworthy item is the system's high participation rate. Taiwan's NHI covers more than 96% of the population and has relieved the financial concerns associated with medical treatment for virtually everyone on the island. This rate far exceeds that of the US, where 14% of the population has no health insurance, and 5.5 million people out of the 13% of the population which has private health insurance have "insufficient coverage."
Not only that, but with approximately 92% of the island's medical institutions having contracts with NHI, care is readily available.
In addition to these widely-recognized points, a lesser-known attribute of the system is its administrative efficiency. The NHI's administrative costs currently account for only 2.3% of its medical expenditures. This is not only below the 3.5% level required by the law, but is also among the lowest of any national health insurance system in the world.
Like a dripping pipe
Unfortunately, behind these successes there lie many problems which require urgent attention.
Huang Weng-hung, an associate professor in the Institute of Health and Welfare Policy at Yang Ming University, says that the current NHI system is like "a leaking pipe." Huang says, "If it is not given a thorough repair, if it is only wrapped up with a strip of cloth or a bandage, one day it will explode."
The biggest threat to the system is that its income is insufficient to cover expenditures. As with the civil servant and labor insurance systems that came before it, NHI, which was established only three years ago, is losing money.
Yang Han-chuan, assistant convener of a workgroup at the DOH, states that NHI's expenditures on medical treatment grew by 13% last year. Revenues from premiums, on the other hand, grew by less than 5%.
As for the current surplus of NT$40 billion that NHI has on its books, Chuang Yi-chou, director of the administrative center at Chang Gung Memorial Hospital and a national policy advisor to the president, says that it was created by overestimates of the average number of dependents per family and by excess contributions from employers. If these mistakes had not been made, not only would NHI not have surplus funds, it would be NT$1.4 billion in the red.
Chuang believes that the only ways to save the NHI system are either to raise premiums, increase the proportion of expenses paid by the insured or reduce waste. "The public and the Legislative Yuan won't support either of the first two methods, so that leaves reducing waste as the only viable solution."
Chang Chin-un, president of the Taiwan Hospital Association, believes that if there is a reasonable distribution of resources and waste is guarded against, NHI would not only not run at a loss, but would have enough funds to lower premiums. "Right now, our premiums are too high!" Chang says that because premiums are too high, it is common for people to under-report their salaries for the purpose of assessing their NHI contribution. According to him, even civil servants are doing so, leading the way in breaking the law.
The sick man of Asia
It is obvious to anyone with eyes that NHI's resources are being wasted and abused. Take the average number of visits to the doctor as an example. Since NHI was established, the average number of visits to a doctor has grown from 10 per year to 14.7 per year, the highest in the world.
"Unless every person is the 'sick man of Asia,' there is no reason for the situation to be this way," says Legislator Shen Fu-hsiung. He says that before NHI was established, labor insurance had become a virutal public feeding trough. In 1994, average annual visits to the doctor under the labor insurance system had hit 15. According to Shen, the overuse and abuse of medical resources now being seen under NHI is much the same thing.
In fact, this waste of medical resources was predicted even before NHI was established. In an attempt to rein in this flaw in human character, some legislators and members of medical associations who recognized the potential problem proposed measures to seal loopholes in the system. The measures proposed included one under which NHI would only have paid for hospital stays, not minor illnesses, and another which would have required patients to pay the cost differential created when they go to a major hospital to treat a minor problem. However, neither of these proposals were accepted.
Shen Fu-hsiung, a proponent of the "ignoring minor problems" approach, asked the Bureau of National Health Insurance (BNHI) a difficult question to illustrate the kind of waste engendered by covering outpatient visits to the hospital: "Which is more important, treating a cold or treating impotence?"
The storm caused by the new impotence drug Viagra is set to strike Taiwan in about six months. If NHI covers one pill per week for Taiwan's estimated one million impotent men, it will cost the system an estimated NT$10 billion per year. "But if NHI pays to treat colds, shouldn't it pay for impotence treatment as well?" asks Shen.
Yang Han-chuan explains: "These measures to close up loopholes are correct in spirit, but are difficult in practice." He says that the civil servant and labor insurance systems that NHI replaced both covered outpatient care. NHI must therefore bear in mind the problem of continuity. It can't start from scratch and not cover outpatient treatment.
Quantity over quality
With no willingness to conserve resources on the demand side, there is no mechanism to force providers of medical care to economize.
A health insurance system can account for medical expenses in any one of three ways. The first method is based on the health of each insured person and on that person's risk factors. This data is used to estimate annual health care expenses and payment is distributed to health care providers in advance. The second method establishes a rates schedule for illnesses, setting a standard rate which is paid to cover treatment of each instance of a particular illness. The third method pays on the basis of actual treatment delivered. Payment is disbursed based upon the kind and quantity of treatment actually given to the patient.
Each system of payment has its advantages and disadvantages. But though virtually everyone agrees that it is most difficult to control costs under the third system, NHI has nonetheless employed it from its inception.
Chen Hsiao-ping, an assistant professor in Chung Cheng University's Institute of Health and Welfare Policy, says that using this method is like giving the medical community a blank check.
And according to Chuang Yi-chou, not one nation which has implemented a national health insurance system using this services-based payment method has been able to run it for long without the government having to take on a portion of its funding. Under a services-based system, doctors have no incentive to conserve. Quite the opposite: The more examinations a doctor gives and the more medicine he prescribes, the higher his profit. This has created a situation in which doctors rake in profits by requiring patients with chronic illnesses to visit the clinic every few days to get their medication and by giving patients with minor ailments all sorts of unnecessary tests.
NHI was initially intended to use a global budgeting system, but this system has proved to be too difficult to implement. However, according to Yang Han-chuan, the BNHI is now working on a pilot program to be tested with dental care in the near future.
Chuang Yi-chou says, "The mechanism is a good one, but the system was designed with the whole nation operating off of one budget. The group covered is too large. It is like cooking rice in a huge pot in that there is no way to control waste." He thinks that the budget should be broken up into smaller pieces for different groups. The only way to make the system work is by dividing it into budgets for the province and various regions, labor unions and hospitals.
"Let's all have a massage"?
In addition to the problem of budgeting, there is the problem of the responsibilities of NHI and other insurance systems not being clearly specified. Taiwan Hospital Association president Chang Chin-un, who also serves as both the president of the Asian Hospitals Federation and as a consultant at Shin Kong Hospital, says that NHI is currently paying for a lot of things that it shouldn't have to, such as occupational illnesses and injuries. In such cases the labor insurance system collects the premiums, but it is NHI which pays for treatment.
Another point which has people worried is the effect of NHI's system of payment on medical care in Taiwan.
By paying for each procedure carried out, NHI is encouraging the medical community to emphasize quantity rather than quality of treatment. It is also encouraging doctors to go into easier fields which pay well. For this reason, dermatology, pediatrics and physical rehabilitation have become hot areas to work in, and doctors are leaving hospitals to set up their own private clinics. On the other hand, more difficult areas of medicine such as surgery are suffering from a shortage of doctors.
Take last year as an example. Physical rehabilitation clinics topped the list of primary care institutions applying for payments from NHI, averaging NT$1.24 million per clinic per month. No wonder people are saying, "Let's all go have a massage on NHI's tab!"
In addition, the payment system, which encourages outpatient treatment over hospital stays (outpatient treatment accounts for about 70% of NHI's medical expenditures), has hospitals earning most of their money from their outpatient clinics, making them less willing to invest in equipment to treat serious illnesses. Chuang Yi-chou believes that if this goes on for much longer, it will lower the standard of medical care in Taiwan.
Privatization
In order to alleviate NHI's many problems, the DOH has proposed privatizing the system. The DOH hopes to reform from the ground up by bringing the private sector, and private sector competition, into the system's operations.
"A cosmetic reform just isn't going to work," says the DOH's Yang Han-chuan. He feels that the constraints imposed on the BNHI by the Central Personnel Administration and its accounting structure have made the bureau inflexible. And because health insurance is a service industry, it requires a certain amount of flexibility to run well. In addition, being essentially a government organ, NHI's supervisory structure is complicated. With so much second-guessing, it is difficult for the bureau to change much of anything.
The idea behind the privatization proposal is to split the BNHI's responsibilities into two parts. Getting people into the program and the collection of premiums would remain unified, but they would be handled by a public foundation. This foundation's board would be comprised of government officials, employers, representatives of the people insured and scholars, and would take over the supervisory functions currently in the hands of the Legislative Yuan.
Management of medical care and payment of expenses, however, would be opened up to private-sector competition among several firms. But to avoid pri-vatization becoming the granting of a monopoly and to keep a check on the system, a government-run insurance organization would be retained.
Can such privatization really bring NHI back from the brink of death?
Huang Weng-hung takes cellular phones as an example of the benefits of privatization involving a number of firms. He says that when the cellular phone market was opened up, competition greatly increased the number of phone numbers available, lowered connection fees, lowered activity fees and lowered prices for the phones themselves. Even Chung Hwa Telecom was forced to improve its service and enter the fray.
But Lin Wan-i cites cable television as a counter-example. He says that the Rebar and Ho Hsin Groups use their control over various cable system operators to fight for market share. As the government has no power to supervise these conglomerates, the consumer suffers.
Set a thief. . .
Hsin Ping-lung, who was asked by the DOH to plan the recent reform proposals, says, "Privatization involving a number of firms will not resolve all of NHI's problems." But he says it will curb waste of medical resources by the supply side, i.e. the medical community.
Because medicine requires a high degree of professional knowledge, most patients are in no position to make judgments regarding the appropriateness of the treatment they receive. With the supply and the demand side on this kind of unequal footing, it is the providers of medical care who decide how medical resources will be used. According to Chuang Yi-chou, the only way to bring these medical resources under control is to put curbs on the supply side.
"The medical marketplace has no vertical integration of upstream and downstream [service providers]," says Hsin Ping-lung. He says that the system is divided into a number of levels, from primary care providers to local hospitals to regional hospitals to medical centers, but lacks vertical integration. As a result, at each level the medications used and the examination departments are replicated.
Chuang Yi-chou estimates that this replication wastes 30% of medical resources. After privatization, each insurance organization would sign contracts with medical care providers to create a medical treatment network. With such vertical links, this waste would necessarily be eliminated.
Moreover, privatization would increase the efficiency of management.
"Those in the private sector have nimble minds," says Chuang. He feels that opening NHI up to privatization would allow private hospitals such as Chang Gung, Shin Kong and Chi Mei to establish insurance organizations to handle management. Chuang is certain that this would be more efficient than a government-run operation.
He makes his point by comparing publicly run hospitals to privately run hospitals. In terms of equipment, private hospitals' costs per bed are 50-60% of those at publicly run hospitals. In terms of patient turnover, too, private hospitals perform better, with a rate 1.5 times that of public hospitals.
But primary care doctors have a different view of the "management efficiency" of corporations. Shih Hsien-yen, director of the Primary Care Association of the ROC, states that if the reforms are approved, "to make profits the corporations will pressure the primary care doctors on the front lines."
Chuang says he can understand the response of primary care doctors, "High numbers of outpatient visits provide primary care givers with more opportunities to provide services. Those who profit naturally protest against reform."
"Set a thief to catch a thief," says Chang Chin-un. Though thieves may not be the most appropriate object for comparison, it is true that it is those on the inside of the medical community who best know how to control medical costs.
Insurance or welfare?
A frequently stressed benefit of the privatization scheme is that it will bring competition into the system.
In Chuang Yi-chou's opinion, insurance and social welfare are two different things. Both provide medical care, but the concept is different. This is evident when you compare England's "National Health Service" to Taiwan's "Bureau of National Health Insurance." If it is an insurance system, everyone should not be treated in the same manner. "Why should all the people of Taiwan have to eat the 'Blue Plate Special'?" asks Chuang. He says that after privatization, fixed rates will push insurers to improve their operational efficiency and offer attractive insurance packages to win new customers.
But Lin Wan-i has doubts about this argument. He says, "Health care is not a product which allows perfect competition." According to Lin, even in the highly commercialized US, the government handles health insurance for the elderly. And in private health insurance for the rest of the population an almost oligarchic situation exists. Large hospitals monopolize the health care market and are moving into areas such as medical equipment and management consulting. The larger they grow and the more services they provide, the higher medical costs go.
Sociologists are concerned that the result of competition for health insurance will not only be the loss of fairness, but also differing levels of treatment based on economic class, and even the monopolization of medical resources by a few conglomerates.
Competition or monopoly?
To ease the public's concerns about privatization, the DOH's Yang Han-chuan points out that after reform, medical services will not be reduced; insurance organizations will not be able to refuse coverage to anyone, and these insurance organizations will not be allowed to earn profits.
Although the proposed regulations state that the private insurers must be non-profit organizations and that their surpluses must be used to increase outlays for medical care or provide more medical services to those they insure, some scholars still have their doubts.
Huang Weng-hung points out that in the past, the records of the DOH's examination of the books of non-profit hospitals were never open to public scrutiny. No wonder the public has no confidence in such regulations.
Moreover, primary care doctors worry that they will lose their professional autonomy with the reforms. Shih Hsien-yen says that with private insurers managing their operations on the basis of earning profits, doctors will be asked to control costs. As a result, the methods and process of treatment and even the medications prescribed will likely be subject to limitations. If this is the case, then we need to be concerned about whether the quality of medical care will be affected.
"The object of the reforms is not to turn losses into profits. It is to provide the maximum amount of service at the minimum cost." But Lin Wan-i believes that letting corporate-backed hospitals become private insurers in order to bring in an element of competition is just too risky.
Economists, on the other hand, feel that having corporations monopolizing the health care market is one of the necessary evils of capitalism. Hsin Ping-lung says: "The public is concerned about the quality of service they receive. What does it matter if there is a corporation behind it? Even more to the point, having a government-run insurer will keep the private insurers in line."
A stage and players
"Privatization is the right direction to be moving in, but it isn't urgent right now. What should be changed immediately is the overall medical environment with its unnecessary waste," states Shen Fu-hsiung. But in his opinion, there is almost no chance of any changes being made to the national health insurance law before the parliamentary elections at the end of this year.
"Who wants to change things now?" asks Chuang Yi-chou. He snidely points out that there is still NT$40 billion in the NHI kitty. Until that is gone, who will want anything to change? The public is in no pain. They're enjoying a health insurance system which is giving them more than they are paying for.
But he warns that three years isn't enough time to reform such a system. "If we can already see the trend, why aren't we moving to give it some serious thought?"
Perhaps operating under the auspices of a foundation can provide the NHI system with a wider stage on which to operate, but the success or failure of the system will still depend on the performances of the players. Chen Hsiao-ping feels that there is still room on the current stage, if only the players will use it. As Lin Wan-i says, the current system hasn't yet been able to achieve targets such as sending patients to particular clinics based on their illness, or creating an overall budget. Given that, he asks why we aren't working for reform within the current system. "From the perspective of our level of skills, reforming the current system is less risky. And when you don't know what the result of reforms will be, you have to be particularly careful."
Be that as it may, as Chuang Yi-chou says, there isn't a flawless system anywhere in the world, and you can't expect reforms to resolve all of NHI's problems. The key is to find a way to create something both fair and efficient in an environment in which resources are limited. This is not just a question for Taiwan, but for the whole world.
p.110
(art by Tsai Chih-pen)
p.112
In the three years since the National Health Insurance (NHI) system was established, large numbers of doctors have been setting up their own clinics in hot areas such as pediatrics, dermatology and physical therapy, increasing the numbers of such clinics by 11%.
p.113
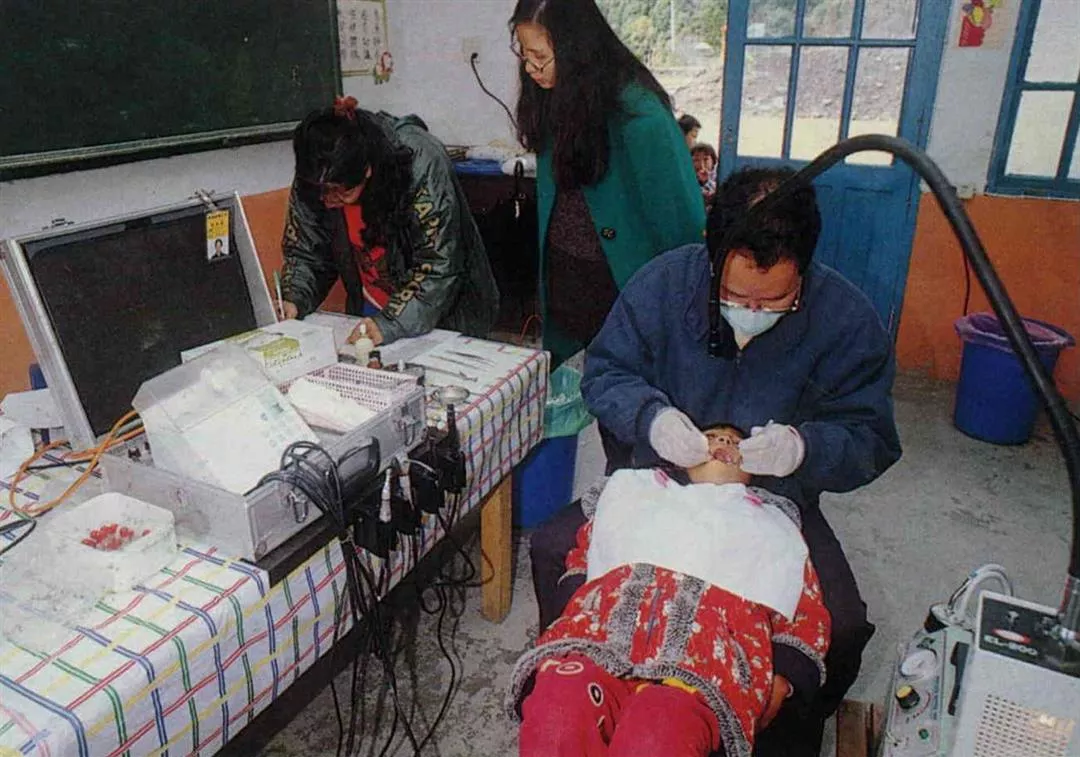
The unfair distribution of Taiwan's medical resources has been a major headache for the NHI system since its inception. How is NHI to raise the quality of medical care for those people living in remote areas?
p.115
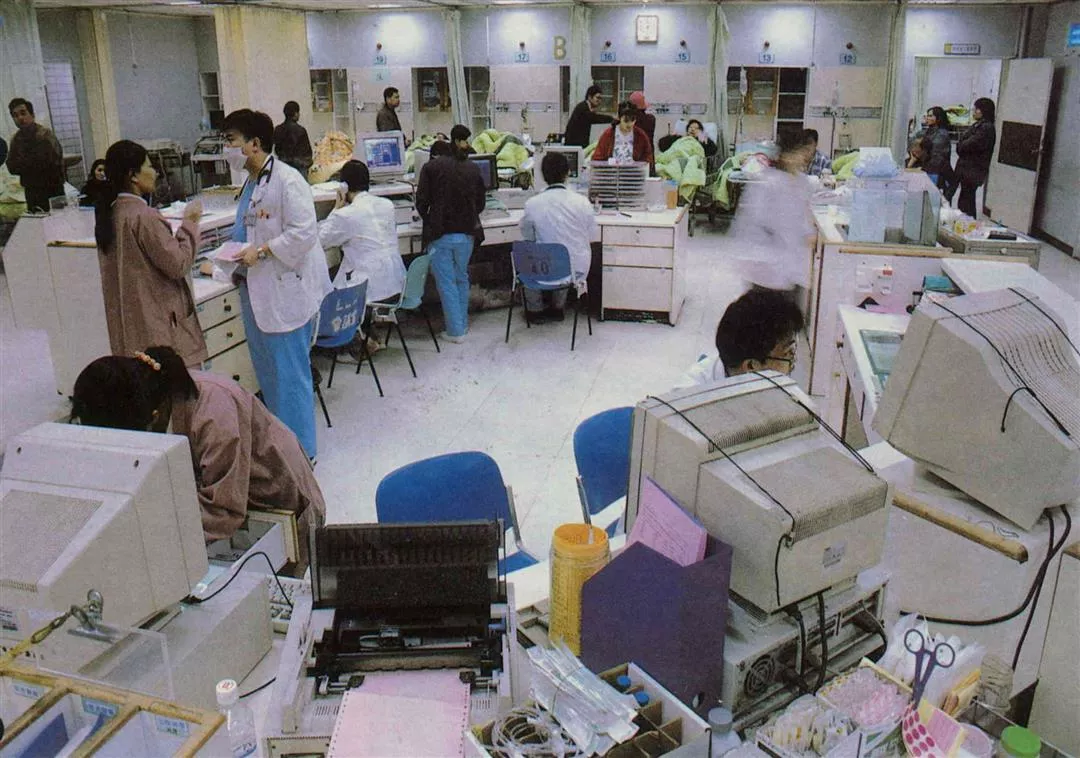
Beds are hard to come by! The NHI's payment system encourages outpatient treatment and discourages hospital stays. The result has been that hospitals are less willing to invest in equipment for treating serious illnesses in their emergency rooms and intensive care units. (photo by Diago Chiu)
p.116
Many are worried that after privatization, those with chronic illnesses will be refused insurance coverage.
p.117
Many health problems require a period of physical therapy after initial treatment, making it one of NHI's greatest expenses.
p.118
Perhaps one of the greatest benefits resulting from NHI is that children, traditionally a "high risk group," now have health insurance. The photo shows the outpatient pediatrics clinic at National Taiwan University Hospital.
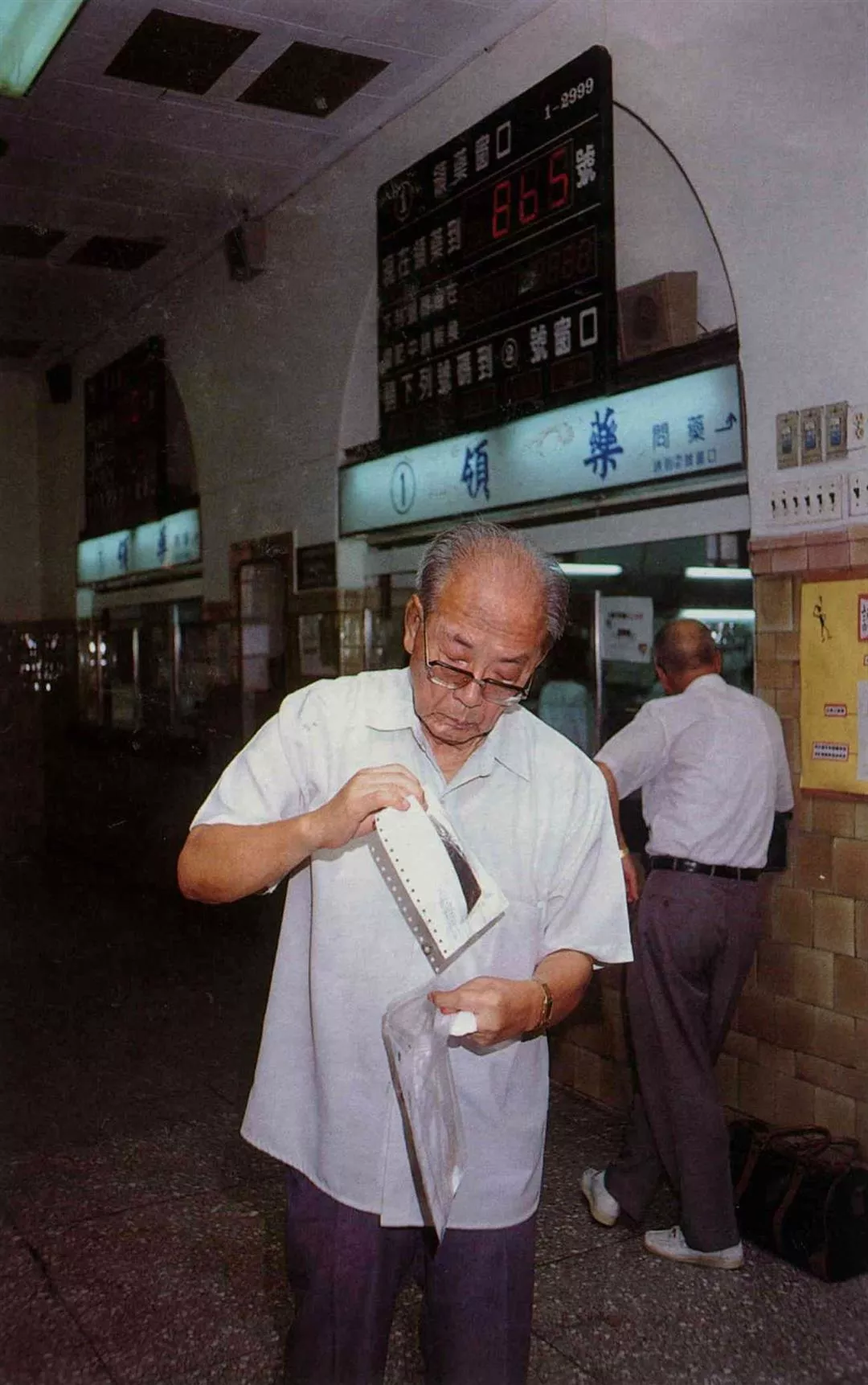
Many are worried that after privatization, those with chronic illnesses will be refused insurance coverage.

Many health problems require a period of physical therapy after initial treatment, making it one of NHI's greatestexnses.

Perhaps one of the greatest benefits resulting from NHI is that children, traditionally a "high risk group," now have health insurance. The photo shows the outpatient pediatrics clinic at National Taiwan UniversityHospital.

@List.jpg?w=522&h=410&mode=crop&format=webp&quality=80)
@List.jpg?w=522&h=410&mode=crop&format=webp&quality=80)




