Recently the world of coronary medicine in the R.O.C has witnessed a series of "great events." First there were two successful heart transplants at the Tri-Service General Hospital and Veterans General Hospital. Then Dr. Cheng Kuo-tsai, D.D.S., returned from the U.S. with the "Phoenix" model artificial heart which he had invented and signed agreements with National Taiwan University Hospital and Veterans General Hospital. Besides transferring the technology, Dr. Cheng has also entrusted the domestic medical engineering world with researching further improvements.
At the end of July, under the joint direction of Dr. Cheng and Dr. Cheng Kuok-kei, Director of Cardiovascular Surgery at Veterans General Hospital, an artificial heart was successfully placed into a pig, opening up a new direction in coronary medicine in the R.O.C.
As the term suggests, an artificial heart fulfills all the basic functions of a normal heart. Its shape copies that of a human heart. The exterior is made of a special plastic; the valve employs a polyurethane material as the base. The heart requires a "heart pump" external to the body to operate, which uses pressurized air to cause the artificial heart to circulate blood.
Although the techniques for transplants of donated human hearts are now advanced, many patients die for lack of suitable donors. At this time, an artificial heart can be used to temporarily sustain the patient until a suitable donor is found. Patients have a fifty percent chance of survival.
After the patient is anesthetized and opened up, and a heart-lung machine is hooked up, the heart is removed and the artificial heart emplaced. Computers and monitors are used to regulate and oversee the changes of the artificial heart.
The main advantage of an artificial heart is that it is less likely to be rejected. But its disadvantages are many.
First, the heart requires two tubes from the chest to a pump which weighs twenty kilograms, so that movement is severely restricted and the chances of infection increased. The patient may "exist," but it is difficult to really "live."
Second, if blood circulates through the artificial equipment for long, the corpuscles may dissolve and lead to hemolysis. And since the surface of the artificial heart is not as smooth as that of the human heart, clots and thrombosis more easily form, leading to strokes. Patients must take anticoagulants. For these reasons the artificial heart may not be used for a long period.
Third, implanting an artificial heart is major surgery, with all the physical and emotional stress and suffering attendant on such an event. Some patients may simply prefer to die; only a very determined patient can survive this ordeal.
The heart that Dr. Cheng has brought back is the small-scale Phoenix model, more suitable to Chinese people. It is about seven centimeters high and its stroke volume can reach ninety cc., suitable for patients of about 65 kilograms. Although Dr. Cheng has had only limited funds to perform experimental implants on animals, and has yet to receive the approval of the U.S. Food and Drug Administration, he confidently says that in concept and structure the Phoenix is not behind the widely used Jarvik model. With sufficient funds and effort, the future of the Phoenix will be bright.
The record survival time for a patient with an artificial heart is 633 days, but the patient still died from infection, stroke, and other complications. Currently great amounts are being invested in the U.S. and Europe to develop an artificial heart. The development of a miniaturized, reliable and permanent portable artificial heart is the next objective.
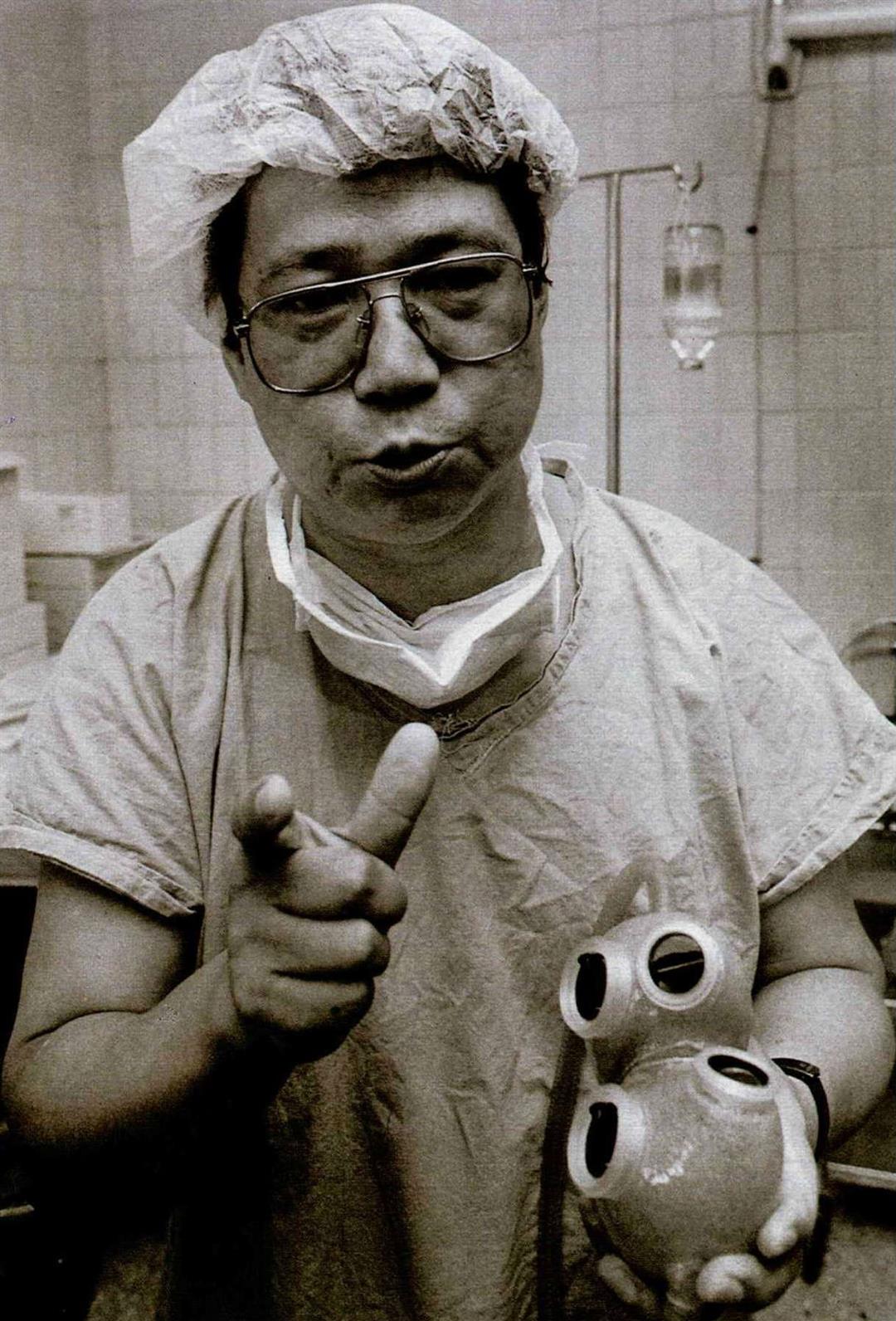
[Picture Caption]
Cheng Kuo-tsai brought back to Taiwan the Phoenix artificial heart which he invented and presented it to the local medical community. (photo by Chang Chia-jung)







