How is SARS classified?
"Better too strict than too lax," is the general rule in preventing the rapid spread of infectious diseases. After the SARS warning was issued, people who had been in a SARS area or who had had contact with anyone or anything having to do with SARS, were classified as "suspected" cases if they developed a fever. If they had abnormal chest radiographs (showing whitish spots indicating the accumulation of white blood cells and body secretions) they were classified as "probable" cases.
According to National Health Insurance records, there are on average 20,000 cases of pneumonia in Taiwan every month. In order to prevent confusing these cases with SARS, an RT-PCR (reverse transcription-polymerase chain reaction) test is now required to make certain that the patient's body does indeed contain the SARS virus.
What is the course of SARS?
The SARS incubation period is from two to seven days, at most ten days.
Based on our current knowledge, during the onset of SARS the virus is busy replicating itself within the cells of the host. There are thus no symptoms nor any ability to infect others. When the virus reaches a certain level, it is then able to break out of the cells and release more virus into the body. At this point the immune system goes into action. The result of the conflict between virus and immune system is a fever, cough and other immune reactions. Thus the disease begins to spread via airborne droplets and physical contact. This occurs when one comes into contact with the oral and/or nasal secretions of the patient or with infected fecal matter and then touches the lining of one's own mouth, eyes or nose. There are no receptors on the skin itself, so becoming infected by skin contact is unlikely.
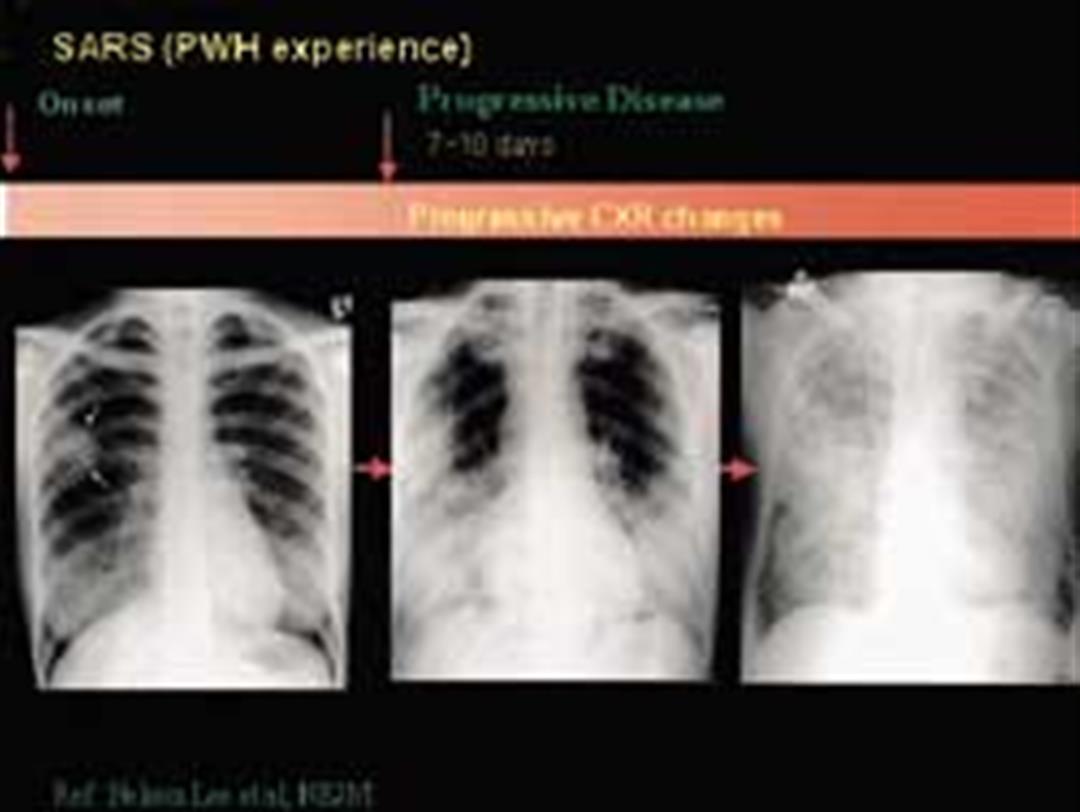
A week after the onset of symptoms the patient's fever can be expected to reach its high point. Thereafter the body learns how to deal with the virus and begins to manufacture antibodies. Affected by the antibodies, the virus begins to diminish to the point where two weeks after the infection begins the majority of patients are almost completely free of the virus. Even if some virus genes remain, they are damaged or barely alive. The antibodies reach their peak three weeks after the onset of infection. SARS lasts about one week longer than the average viral infection.
Is SARS incurable?
The SARS virus is by no means difficult to kill. But why, then, is the case-fatality rate of the disease as high as 10-20%, fully 100 times more than the average influenza with a rate of 1 in 1000?
The current thinking is that what kills a person is not the SARS virus itself but the immune reaction of the patient's own body. In order to fend off this foreign invader, the immune system moves into high gear. White blood cells and lymph cells move in great number into the lungs to combat the virus and create what is called the "cytokine storm" that causes serious inflammation and damage to the lung, even leading to pulmonary fibrosis. The lungs' air sacs, originally fluffy and soft, become as hard as stone and the patient dies from respiratory failure.
According to the data, aside from persons suffering from chronic liver, lung and kidney diseases and the old and infirm, those who exhibit the most severe symptoms are adults aged 20 to 50. Conversely, children whose immune system has not yet fully developed are able to escape this scourge. This provides evidence for the inference that it is the reaction of the immune system and not the SARS virus itself that kills a person.
To date there is no standard treatment for SARS. To raise the survival rate doctors may give antiviral agents such as ribavirin and interferon during the initial stage of infection thus preventing the initial massive replication of the virus in the body. During the middle stage of the disease, to prevent the patient's immune system from becoming over-stimulated, it is necessary to administer steroids and immunoglobulin to weaken and adjust the immune reaction. A tough question is whether, once the immune reaction has been thus weakened, this will allow other microbes to take advantage of the situation and attack. Experts relate that the disease shows rapid and unpredictable changes in symptoms and severity in different patients, making treatment especially difficult.
In the latter period of the disease, many patients may undergo the painful stage of "intubation" (a breathing tube is inserted directly into the lung through the throat to aid breathing). Aside from meticulous care and excellent supportive treatment, it appears in the end all the patient has to depend on is the will to live and "luck."
Unfortunately, the viral infection frequently leaves scars for a lifetime. Some SARS patients who have survived their ordeal will nevertheless live their lives out with lungs damaged by fibrosis. What is even more worrisome, just like after the "Spanish influenza" of 1918 swept the globe, some patients have shown a peculiar and frightening after-affect-sleeping sickness. Some experts also now suspect that the SARS virus may invade the brain and cause neurological damage.
What factors affect severity?
Some people who contract SARS have mild symptoms. They show fever, have chills for a few days and then get better. Others contract the disease and die within a very short time. What is the key difference? Experts conjecture that the amount of the virus one is initially exposed to seems the most significant factor. But because the SARS virus mutates frequently, is it possible that some viruses just become more severe, more virulent the more they mutate? The scientific world is not discounting this possibility but to get a clear understanding of the situation will probably take quite a while.
In addition, examination of specimens from two severely affected patients, the younger brother of Mr. Tsang from Block E of Hong Kong's Amoy Gardens apartment complex and Ms. Tsao from Hoping Hospital, revealed the presence of two other common culprits of bacterial pneumonia in addition to the SARS virus. These were Chlamydia and Mycoplasma. This type of combined, multi-pathogen infection seems to be a reason for the aggravation of a patient's symptoms.
The SARS epidemic began in Guangdong and so has also been called the "Chinese plague." In Canada and Vietnam the epidemic is already on the wane. From a global perspective, only China, Hong Kong and Taiwan remain locked in a vicious struggle with this curse. Is it possible that the SARS virus is "partial" to Chinese? Though researchers are exploring the link between SARS and human leukocyte antigen (HLA) in persons of Chinese ancestry, experts say a virus might very well select certain "physical types" as a host but certainly not any particular "race."


@List.jpg?w=522&h=410&mode=crop&format=webp&quality=80)
@List.jpg?w=522&h=410&mode=crop&format=webp&quality=80)




@List.jpg?w=522&h=410&mode=crop&format=webp&quality=80)