7S breast reshaping
Breast reconstruction is divided into two types. The first is implantation of prosthetic material. The second is transplantation of tissue from elsewhere in the patient’s body (“autologous tissue”), with several variants depending upon the source of the transplanted tissue. Is any one option better than the others?
“By no means is the same approach suitable for every patient,” says Tang Yueh-bih. Breast reconstruction must take into account the “7S” factors: size, scarring, shape, softness, symmetry, silhouette, and simulation of the nipple-aureole complex. It is necessary to weigh the unique situation of each patient, and design a reconstruction approach tailored to the individual.
Implantation of prosthetic material is the simpler method. It only takes about an hour of surgery to implant a saline water bag or silicone gel. Moreover, this method is cheaper and doesn’t require scarring any other part of the body. But there are quite a few drawbacks as well: possible rupture of the implant, capsular contraction, infection, hematoma, and lacking the texture and flexibility of a natural breast.
As for reconstruction using autologous tissue, the tissue can come from several different places in the body, including the back, buttocks, thigh, or abdomen. Scientific names include the latissimus dorsi flap, pedicle transverse rectus abdominis myocutaneous flap, deep inferior epigastric artery perforator (DIEP) flap, and superior gluteal artery perforator flap. Each source area has different pros and cons.
Early on, autologous tissue transplants were mostly done using the latissimus dorsi, borrowing tissue from the muscle in the back that controls shoulder movement. This technique has always enjoyed a high success rate and rapid patient recovery. But because there is not much excess material in the latissimus dorsi, removing it leaves the patient subject to reduced shoulder mobility, while the reconstructed breast is less soft to the touch and more likely to contract in size due to inadequate blood supply.
Professor Cheng Ming-huei, chief of the Division of Reconstructive Microsurgery in the Department of Plastic and Reconstructive Surgery at Linkou Chang Gung Memorial Hospital, says that at present the method that “entails the fewest costs and offers the greatest returns” is the DIEP flap approach. Cheng, one of the world’s leading breast reconstruction specialists, has published 32 papers on the subject in international journals and conducted nearly 1000 procedures, of which 464 have been done using the DIEP flap method, with a success rate of 98%.
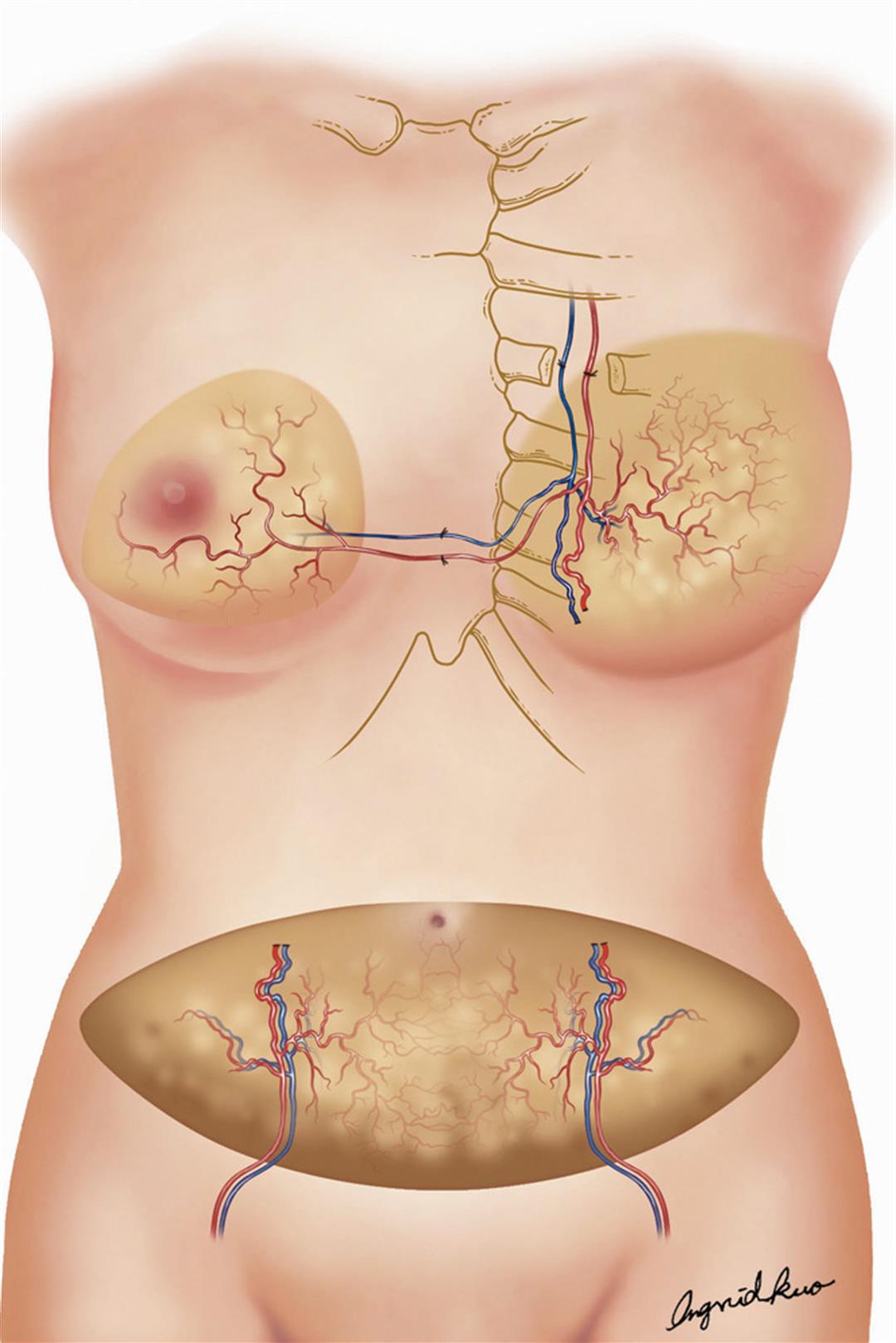
The DIEP flap method entails removing a layer of adipose tissue (fat) roughly 12 x 30 centimeters in size from the abdomen, along with the skin and the blood vessels, and transplanting this material into the chest area. Microsurgical techniques are then used to connect the blood vessels with the intermammary artery, so that the transplanted material survives as living tissue.
Cheng says that it used to be the case that abdominal muscle was transplanted along with the adipose tissue. But this often led to side effects like hernia and weakness in the abdominal region. Today, only the fat is taken, while the muscle is left behind.
It’s especially exciting that the reconstructed breast is “alive.” It has a natural shape and the same feel to the touch as a real breast, and when the nerves grow in after about half a year, there is sensitivity in the breast as well. And as an added bonus, you get a smaller tummy without having to do any dieting or exercise!
It is worth adding here that Cheng has drawn on his tremendous surgical skills to invent his own nipple reconstruction technique. He takes a centimeter of cartilage from the patient’s third rib and inserts it under the skin. About half a year later he then refines it into an upside-down T shape to serve as a nipple. Finally, he injects colors into the skin—using tattooing skills he learned especially for this purpose—to create a natural-looking nipple and aureole.
The third option
Breast reconstruction techniques are getting more sophisticated every day. But still many patients—because of financial considerations, a risk-averse mindset, or fear of pain—are not willing to go through a second reconstructive surgery after the initial mastectomy.
Lin Wei-chieh of the Taiwan Breast Cancer Alliance prefers to wear a prosthetic breast rather than undergo reconstructive surgery. “A lot of doctors skip over the part about how much it hurts,” says Lin. Of course everyone would like to look perfect, but she just doesn’t have the courage to go through the pain of surgery again.
In some cases, where enough of the breast can be saved so that there is no need for a full-scale breast reconstruction, it is possible for the surgeon to do a cosmetic procedure at the same time as removing the tumor, to leave the breast with a reasonably natural appearance after surgery.
Hsieh Chia-ming, head of a task force at Taiwan Adventist Hospital specializing in breast cancer, notes that in the past when doctors were able to remove a tumor while conserving most of the breast, the breast was left misshapen. In recent years he has borrowed techniques previously used for cosmetic breast surgery to shift remaining tissue in the affected breast around so as to leave the individual with a more balanced and more natural appearance. Hsieh has used this procedure in 130 cases in recent years, and patients have expressed a high level of satisfaction.
However, Hsieh reiterates that this method is only for certain types of cases. Candidates must be in the early stages of the disease, with only a single tumor or closely neighboring tumors. Also, the patient must have sufficient breast density, and the tumor(s) cannot amount to more than 20% of the breast tissue by volume. Otherwise the procedure will not be very effective.
The joy of restitution
According to a report based on a 2005 survey conducted by the Taiwan Breast Cancer Alliance, more than 90% of respondents were aware that the option to have reconstructive surgery existed. But only about 5.6% had chosen at that point to have the procedure, a much lower percentage than in the US (25–30%). The most important reason is probably that breast reconstruction is not covered by National Health Insurance in Taiwan, so must be paid for out of pocket. Not many people can afford the NT$200–300,000 that the surgery costs.
Cheng Ming-huei says that in the US, breast reconstruction is considered to be part of the treatment of the cancer, and in fact, under a 1998 federal law, insurance coverage is mandatory. In recent years, thanks in part to efforts by the Taiwan Breast Reconstruction Association to promote the procedure, the ratio in Taiwan has been gradually climbing. For example, today over 10% of women admitted to Chang Gung Memorial Hospital for breast cancer treatment opt for reconstructive surgery.
Besides cost, another critical variable is family attitudes. Sometimes families feel that it is unimportant for an older woman to retain this “secondary sexual characteristic.” But Hsieh points out, “No matter how old you get you are still a woman.” Unfortunately children who make treatment decisions on behalf of elderly women rarely can understand what it feels like for their mother, for whom the loss of a breast is “mourned.”
“Family support is very important,” says 46-year-old breast cancer patient Liu Fengyu. For a while after her surgery she was deeply depressed and wouldn’t even go out of the house, until her husband finally told her: “Whatever you think is best, go for it!”
Liu recalls: “The first time I looked in a mirror and saw my reconstructed cleavage, I began to feel happy from somewhere deep inside, and I just couldn’t stop smiling!” Her husband and friends also noticed how upbeat she became after the reconstructive surgery.
Chen Wenjuan, a past director of the Taiwan Breast Reconstruction Association, says that just having reconstruction as an option gives hope to patients, helping them summon up the courage to face a mastectomy, and to cope with all the follow-up treatment. The knowledge that they could be restored to their original appearance is what saves them from being “haunted” by their illness.
Septuagenarian Luo Lirong, in the vanguard of women who have had breast reconstruction surgery, says: “I hope that all women who have lost a breast will one day be able to enjoy the pleasure of ‘restitution’!”



@List.jpg?w=522&h=410&mode=crop&format=webp&quality=80)






@List.jpg?w=522&h=410&mode=crop&format=webp&quality=80)