It's all about leverage
Could the two surgeries be combined into one, to reduce the time under the knife to the minimum? This was the key problem that Dr. Chang, who has been in practice for 27 years, finally cracked in 2003.
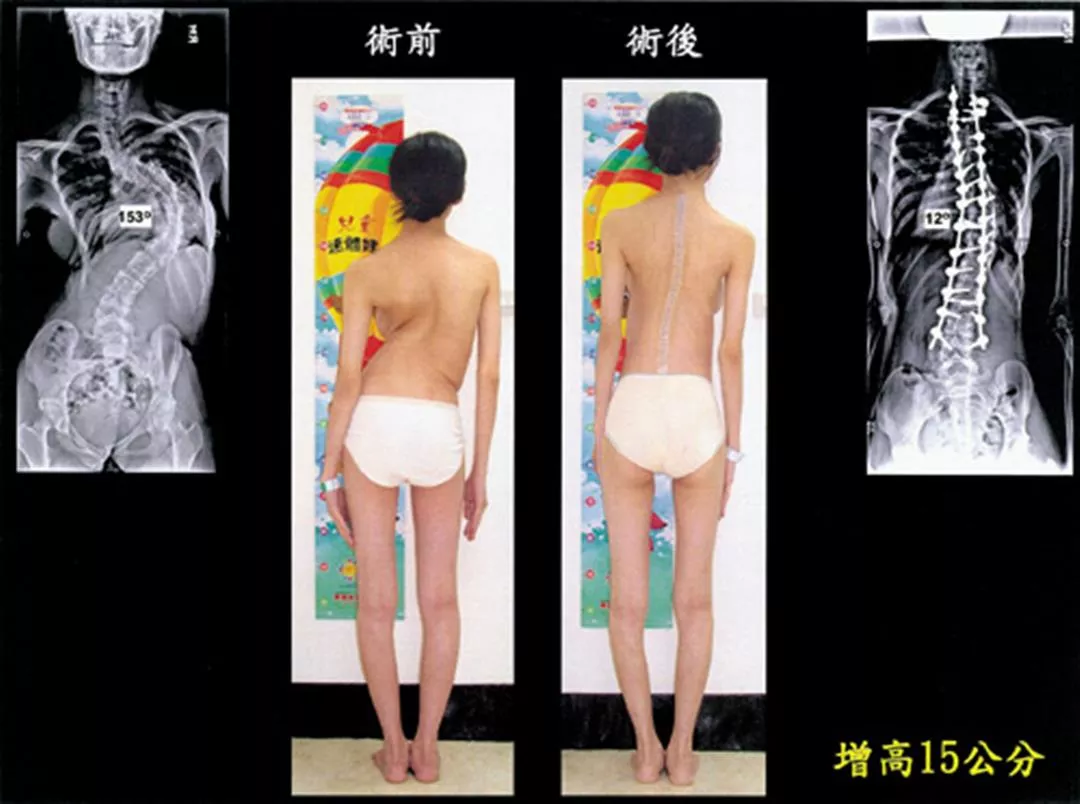
On a typical day when he does not have clinic hours, the 56-year-old Chang Kao-wha is just coming out of surgery at 2:30 in the afternoon, having done three successive operations starting early in the morning. This is his first chance to grab some food and take a break. Heading into his office, he opens a report on his computer screen and looks over some pre- and post-operative photos and X-rays of a patient he treated who had a curvature of 153 degrees in her thoracic vertebrae. The images (see p. 102) are rather shocking at first glance.
In a photo of the patient's exposed back before surgery, you can see that her two shoulder blades were clearly uneven, with the left shoulder being five centimeters lower than the right. Because her thoracic vertebrae were distorted toward the right, the muscles in the lower left portion of the thoracic cage, lacking support, had collapsed severely. On the right side, the area beneath the waist near the hip bone also showed collapse inward. The patient's cardiopulmonary system did not function well, and she would rapidly get out of breath just by walking. Even worse, because the spine pressed down on the nerves, she felt pain, numbness, and weakness in her lower limbs.
"The patient's spine and muscles were originally badly twisted, but after surgery they were corrected to become straight and even, even making the patient 15 centimeters taller, just like an ugly duckling turning into a swan! The space for internal organs was also expanded and her cardiopulmonary function improved." This is the result of the "cantilever bending technique" that allows patients to be completely transformed.
Each operation of this type begins with Chang leading a team of 24 in preparation of an electrical saw, drill, hammer, steel pins, steel wire, and other materials and implements. Lined up ready to go, they look very intimidating.
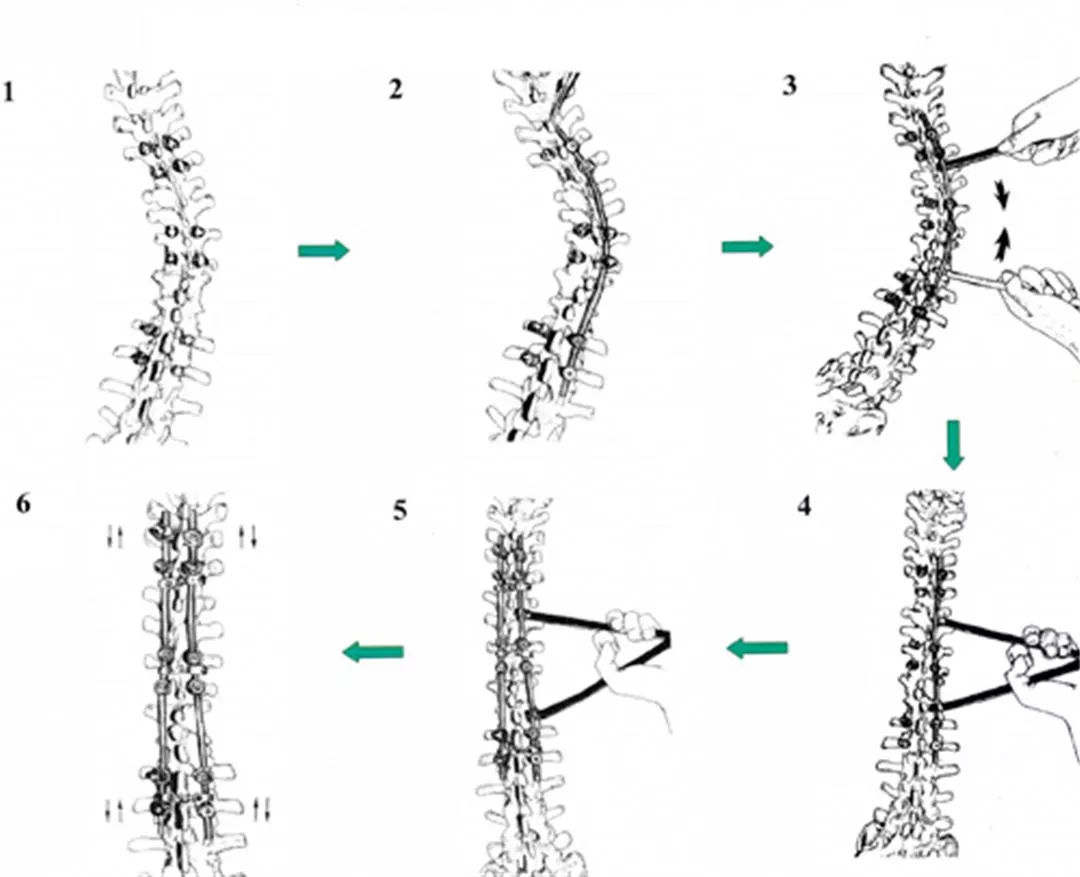
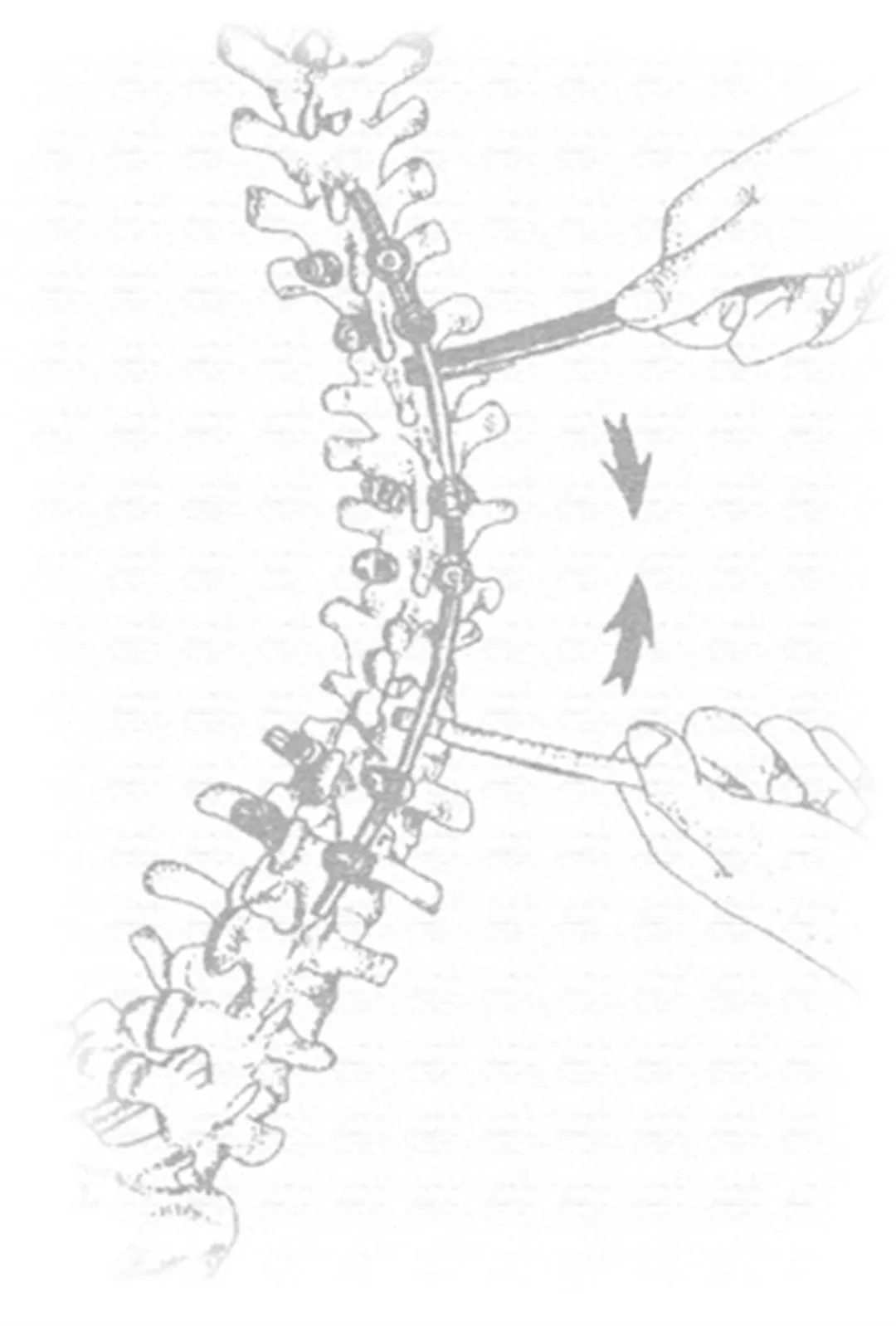
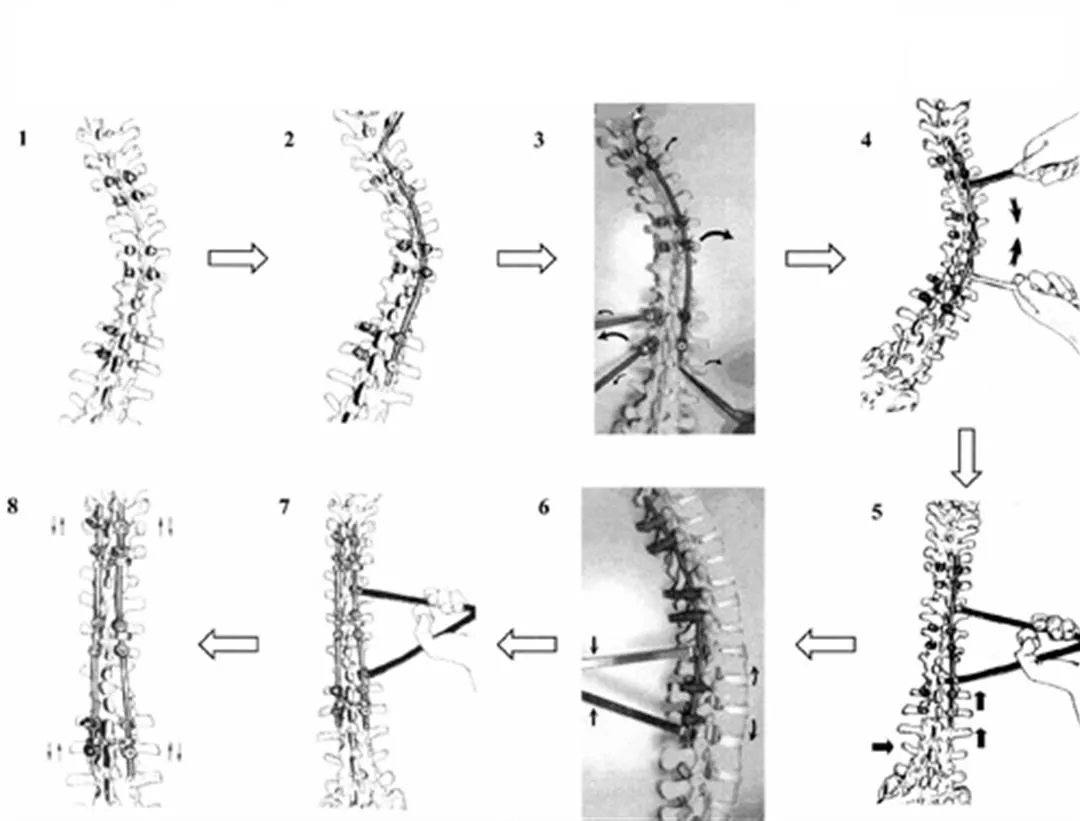
The surgical procedure is as follows: An incision is made in the back, and the muscles surrounding the vertebral column are pulled away. Then a drill is used cut holes in the pedicles of a number of vertebrae for insertion of screws. (For example, the patient with a curvature of 153 degrees had 28 metal screws inserted.) Then thin metal rods are used to link the screws and fix them tightly, after which a cantilever is used to gently align each out-of-place vertebra. Finally, the rod on the other side is locked down, thus providing two stable metal tracks, creating a pillar of support for the newly straightened spine. (See illustrations.)
"The cantilever is very strong and provides a lot of support. As for how much force you have to apply and how many vertebrae have to be aligned, you can't know that for sure until the surgery itself. Also, the number of screws differs case by case." For example, Chang explains, one patient had a spine that had curved into an S shape. The deformation was composed of three curves, so it was necessary to insert over 20 screws from the first thoracic vertebra to the third lumbar vertebra in order to get a satisfactory correction.
The greatest difficulty in the cantilever bending technique is that getting the angle and amount of force right when putting the screws into place depends entirely on "touch." Yet there cannot be even a millimeter of deviation, or you will damage the spinal cord, which is as fragile as a piece of tofu. "For most spinal surgery you can be guided by X-rays, but for patients with severe deformations, the nerves and blood vessels are also abnormally twisted. So you can't rely on the help of technology, you have to go by feel," stresses Dr. Chang.
In November of 2003, Chang published a paper in the international orthopedic journal Spine discussing 41 cases he had treated using the cantilever bending technique in a five-year period from 1998 to 2003. The average curvature for these 41 patients was 98 degrees (ranging from 75 to 133 degrees), with average post-surgery correction being 67%. Not a single patient had post-operative complications, and 38 of the patients expressed themselves "extremely satisfied," while the remaining three said they were "partly satisfied." These figures indicate that his surgical technique was quite successful.

A patient who has undergone corrective spinal surgery can usually be out of bed by the third day, but he or she needs to wear a brace and do physical therapy for six months in order to allow the skeleton to properly heal.




@List.jpg?w=522&h=410&mode=crop&format=webp&quality=80)






@List.jpg?w=522&h=410&mode=crop&format=webp&quality=80)