Not miniature adults
Not only are common childhood illnesses different from common adult illnesses, but even the same illness exhibits different symptoms and courses in children and adults.
Urinary tract infections are common in diaper-age children. But whereas in adults the typical symptoms (painful, urgent, and frequent urination) make it easy to diagnose such infections, in infants and toddlers the typical symptoms (fever, irritability, vomiting, and diarrhea) appear to be completely unrelated to the urinary organs. If the physician is not alert to this, he can easily mistake a urinary tract infection for a common cold or gastroenteritis.
Myocarditis, a condition that is often seen in children and can easily result in medical malpractice disputes, is also difficult to diagnose. Huang Fu-yuan explains that one of the early symptoms of myocarditis is fever, which is also typically associated with the common cold. A general practitioner who neglects to listen carefully to the child's heart while conducting the diagnostic examination can easily miss this disorder. Unfortunately, because myocarditis is a rapidly progressive condition, even a small delay in treatment can easily prove fatal.
In other countries, it is a matter of course that a child who falls ill is taken to see a pediatrician. In Italy the law requires that children under six be treated by pediatric specialists. But in Taiwan, it is commonly believed that anyone who has a medical license is a doctor and that's that; in other words, it is assumed that not just pediatricians, but ear, nose and throat (ENT) specialists, family practitioners, gastroenterologists, and dermatologists are all qualified to treat children.
According to Taiwan Pediatric Association statistics, approximately 40% of Taiwanese children under three have seen a pediatrician, 30% an ENT specialist, and 20% a family practitioner.
The "chaotic state" of front-line medical practice greatly increases the risks of children's healthcare. "ENT specialists can only examine and treat part of a patient's body. Because they rarely examine a child from head to toe, they cannot identify and diagnose problems outside their field of expertise. Family practitioners receive only three short months of pediatric training in medical school and may never even have come across a serious childhood illness such as an enterovirus infection. How can they be expected to make correct diagnoses?" asks Huang Fu-yuan.
"The more you see, the scarier it gets," says Lin Tzou-yien. Children are full of vitality and have a fast metabolism, but they often get violently sick and when they do, the illness can progress so quickly that it has to be monitored from hour to hour. Reye's syndrome (a form of encephalitis of uncertain cause which usually occurs after viral infections) often deteriorates to a coma within a few hours of onset. There have also been many cases of severe enterovirus infections that resulted in death within 24 hours of hospitalization. The initial symptom of meningitis is a temperature very much like that associated with a cold, but within one or two days the patient's condition can take a dramatic turn for the worse. Many parents who lose a child accuse the doctor of misdiagnosis because they don't understand that it is quite possible for a child to be playing happily one minute and fall ill beyond recovery an hour later.
You get what you pay for
"During each stage of their children's development--which happens very fast--it is very important for parents to have them vaccinated, give them proper nutrition, and educate themselves about the growing process," says Lin Tzou-yien. He stresses that only when the prevention and treatment of childhood diseases is integrated and pediatricians do timely public health education work will comprehensive children's healthcare be achieved.
So much for the ideal, but "the biggest obstacle is a lack of resources," says Huang Fu-yuan, hitting the nail on the head. Huang points out that children's hospitals in Europe and North America can count not just on income from insurance companies but also on very generous donations. Big-name movie and sports stars organize benefits to raise money for children's hospitals, while visiting royalty and heads of state are sure to be taken to see them. In Japan, insurance companies pay hospitals 26-48% more to treat a child than they do for an adult undergoing the same treatment. By comparison, children's healthcare gets short shrift in Taiwan. Particularly since the "global budget" system (in which hospitals receive lump sums from the NHI program to cover their medical expenses for each fiscal year) was introduced in 2002, children's healthcare has been squeezed for funds.
Because children tend to cry and are difficult to control and communicate with, providing outpatient pediatric services is more demanding and requires a higher investment in time and personnel. For example, an electrocardiogram or an echocardiography can be performed in ten minutes on an adult, but it may take more than 40 or 50 minutes in the case of a child. Such problems result in higher costs that are not reflected in the payments received for the treatment.
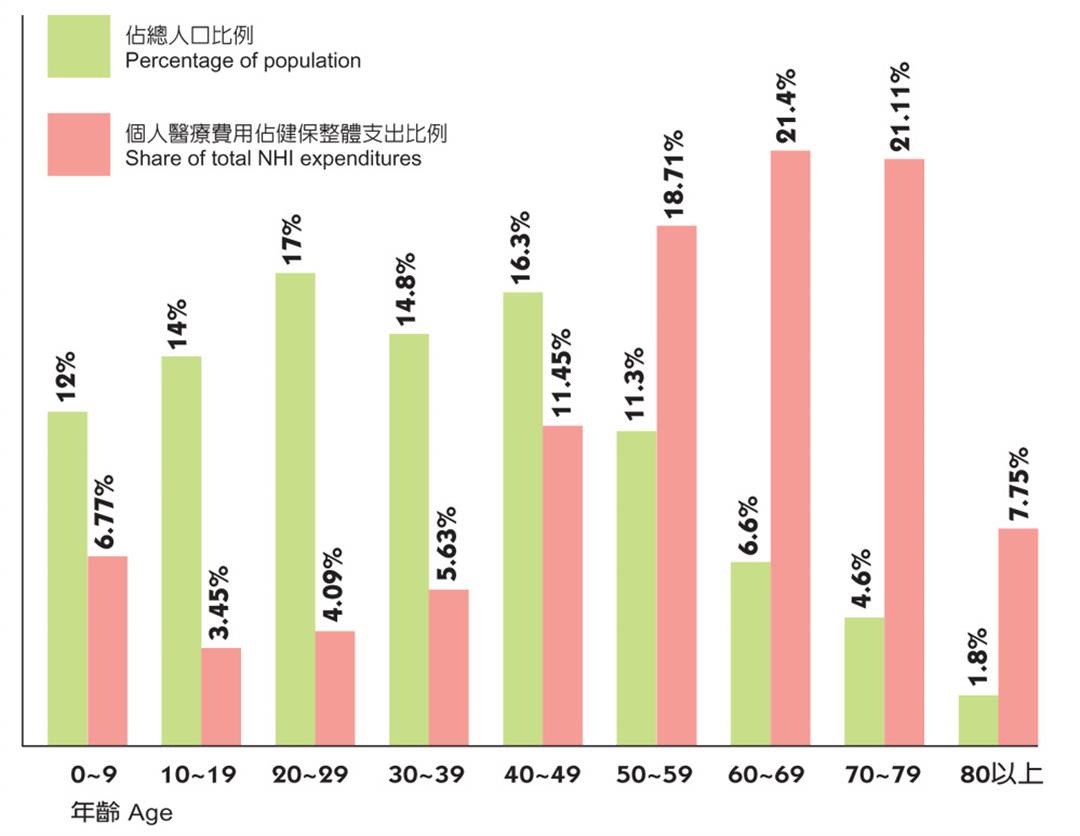
Huang Fu-yuan notes that children under 18 comprise 26.7% of Taiwan's total population but only 12.5% of NIH payments, which is less than is spent on dialysis. On the other hand, the 9% of people who comprise the elderly population use up 33% of NHI payments. "More than half of healthcare expenditures are made in the six months prior to death," says Lin Tzou-yien, who asks whether a under a system and mindset that "cares more for the dying than the living" the masters of the nation's future are receiving woefully inadequate medical care.
The last straw?
A new NHI payment system will be introduced in January 2008 which will put patients into diagnosis-related groups (DRG) irrespective of individual differences. For many financially strapped hospital pediatrics departments, this may well turn out to be the straw that breaks the camel's back.
Pediatric medicine has always been a drain on personnel and financial resources. Many big hospitals are unwilling to invest in pediatric departments and even university medical centers do not necessarily have a full range of pediatric equipment. It is no more reasonable to ask a toddler to wear adult shoes than to force children to share X-ray and electrocardiogram machines with adults, but that is precisely what is happening. Doctors who have to deal with life-and-death situations can only stomp their feet in frustration.
"Even the country that spawned the ill-advised DRG system--America--does not include children's healthcare in it," says Lin Tzou-yien bluntly, adding that this kind of system can create a situation of "selective healthcare." In the future, warns Lin, cases such as that of "Little Sister Chiu" (a four-year-old girl who died after being turned away by several hospitals following a severe beating by her alcoholic father) will occur again and again in Taiwan. This is particularly true in the case of critical-care medicine that involves high human and material costs and long-term care. For example, there will not only be a lack of money and doctors to treat major childhood diseases, congenital anomalies, and septicemia, but even research and teaching in these areas will take a big hit.
Besides the fact that when the NHI system was introduced, no thought was given to the special characteristics and problems of children's healthcare--an omission that has resulted in underfunding in pediatric care--in recent years Taiwan's birthrate has registered a rapid decline. Last year, for the first time, the number of births fell below 200,000. The children's healthcare market is shrinking and pediatricians are grumbling. The number of primary pediatric clinics has fallen from more than 100 during their heyday a decade ago to fewer than 30 today. Even in big hospitals, pediatricians have had to accept salary cuts. As hospitals have come to consider pediatric care a losing proposition, pediatricians have become second-class citizens in the medical community.
Fewer choose pediatrics
"The fuse is burning short," says Huang Fu-yuan, and no one in pediatrics knows where the money is going to come from. The Department of Health approved an upper limit of 240 new pediatric residents this year, but so far fewer than 100 have been recruited. Each hospital can only afford to recruit 40% of the pediatric residents it needs and has to make up for the staff shortage with nurses. Lin Kai-hsin feels very strongly about this. He says that most pediatric residents choose less demanding specialties. It has been several years since anyone specializing in his own field of pediatric hematological oncology (leukemia) was hired.
Because children's diseases are highly volatile and frequently lead to malpractice disputes, pediatricians are always watchful of possible pitfalls and fearful of making mistakes. They also face enormous pressure from unreasonable parents who demand that they immediately bring down their child's temperature, call them at the slightest hint of illness, and insist that they be on call at any hour, never allowing them a moment's rest. For these reasons, many newly graduated pediatricians throw in the towel after six months and change to a less demanding specialty.
The market is shrinking and pressure is growing. The fact that fewer and fewer medical students are choosing pediatrics as their specialty seriously threatens the future quality of pediatric medicine in Taiwan. "Unless we figure out a way to remedy this situation, we risk destroying the foundations of our country," warns Lin Tzou-yien.
Children are the adults of the future. A healthy citizenry tomorrow depends on healthy children today. Children are full of vitality and have a remarkable capacity to recover quickly from most illnesses, but although pediatric medicine is demanding and costly, no matter how we figure it, offering children good healthcare wherever they live is an investment the nation and society cannot afford not to make.





@List.jpg?w=522&h=410&mode=crop&format=webp&quality=80)
@List.jpg?w=522&h=410&mode=crop&format=webp&quality=80)




