Medicine vs. Human Right--Where Should the Balance Lie?
Chang Chiung-fang / tr. by Jonathan Barnard
January 2008

Everyone should be able to enjoy medical care. It is a basic human right. Yet is it possible both to push for medical progress and to respect human rights? The question is getting harder and harder to answer.
From SARS prevention measures, reproductive technologies and prenatal screening and testing, to notification about medical conditions, near-death resuscitation, clinical trials and biological databases, a growing number of medical issues involving human rights have cropped up in recent years amid constant global change. Some of these controversies stem from using people as stepping stones for medical progress; others are connected to dilemmas and struggles that have occurred in the wake of advancing medical technology; and still others hinge on conflicts between the greater social good and individual rights. Pitfalls are impossible to avoid. These difficult issues have reached a critical point where they can no longer be ignored and deserve everyone's attention.
"In my father's era, before the use of antibiotics, general anesthetics, or surgical gloves, doctors could be described as being in a constant bloody struggle to save the lives of pregnant women and babies." In his book The Ivory Tower: Sixty Letters to a Medical Student, Hsieh Fon-jou, a professor at National Taiwan University's College of Medicine, thus recalled the insufficiencies of medical resources and care during an earlier era of medicine in Taiwan. (His father began working as an obstetrician in the 1940s). "In his mind the concept of 'ethics' didn't exist. He simply based his actions on the idea that doctors ought to save lives." The doctor-patient relationship back then was much simpler and more relaxed than it is now.
But the good old days aren't coming back. Medical technology has been steadily advancing. It now not only provides treatments for illnesses, but has even, in some cases, allowed man to become master of his own fate and declare war on all kinds of "incurable" diseases. But at the same time there is growing consciousness about human rights, so that the ill are no longer powerless beings and doctors are no longer given carte blanche to make medical decisions and perform research as they see fit. Increasingly the doctor-patient relationship is one where the two parties are at each other's throats, as medical progress and human rights seem to be at loggerheads.
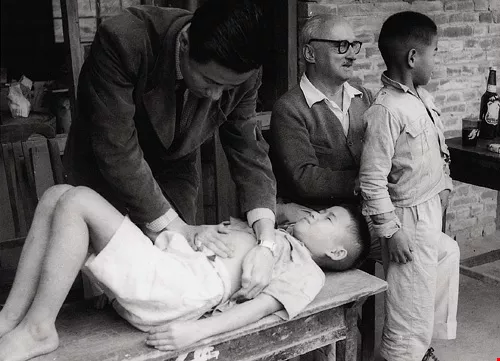
In the first few years after Japan's surrender of Taiwan, health, hygiene, and medical conditions were poor, with contagious diseases widespread, and foreign medical and charitable groups dispatched personnel to help the Taiwanese people. Today, facing new contagious diseases, people are both afraid for themselves and concerned that their rights should be protected.
Life and death decisions
In recent years reproductive technologies and prenatal screening are the areas of medicine that have raised the most red flags when it comes to human rights.
Surrogate mothers, sperm banks, egg donation, test-tube babies and other artificial reproductive technologies have provided women with greater reproductive freedom. On the other hand, in conjunction with surviving myths about the importance of providing heirs to carry on the family line, the advancement of reproductive technology and the introduction of new drugs and medical equipment have turned women into reproductive machines. Their bodies are being used and manipulated more than ever.
"For women, does the advancement of reproductive technology ultimately represent liberation or exploitation?" asks Rei Wenmay of the Institute of Public Health at National Yang-Ming University. She observes that most people look only at the hope that reproductive technologies bring to those who cannot conceive, but very few look at the damage they can do to women's bodies, including the pain from administering fertility drugs and egg retrieval. And because the success rates are only 20-40%, such interventions lead to great anxiety and depression among those women who still can't conceive.
Whereas reproductive technologies end up limiting women's freedom over their own bodies, prenatal screening damages an unborn child's right to life.
The Genetic Health Act of 1999 allowed prenatal screening for deformities, hereditary diseases (such as thalassemia), and genetic diseases (such as Down's syndrome). It also gave parents the authority to choose to "prevent a human tragedy." Meanwhile, medical technological progress has allowed tiny babies of less than 1.5 kilograms to survive. Yet, because their organs are not fully mature, they frequently suffer from problems with the respiratory tract, hearing, retina, and nervous system. Future medical troubles are a certainty.
The advance of medical technology has replaced a "decision of God" with a "decision of man." This has extended the lives of many newborns who were not ready to live outside their mothers' wombs. But it also raises questions: Who should be allowed to decide about life and death? What criteria should be applied when making these choices?
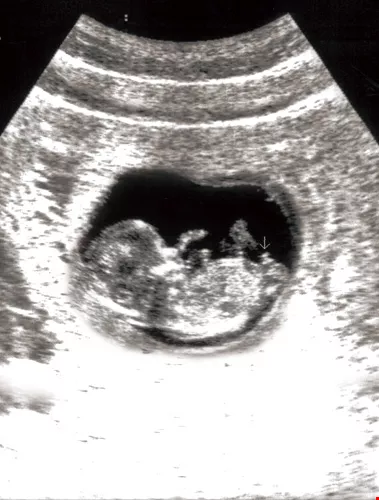
Pre-natal screening and other developments in reproductive technology can help avoid the transmission of serious genetic diseases, while also offering greater reproductive freedom to women. However, it also raises questions over the fetus' right to life.
Made-to-order babies
"Parents can make a decision about whether or not they should give birth, but that shouldn't be at a cost of sacrificing their respect for life," says Rei Wenmay. She cites abuses of prenatal screening: some people, merely because of dissatisfaction with a fetus's gender, cleft palate, or so forth, have abused the intent of the Genetic Health Act and made a decision to extinguish an unborn child's life. There have also been cases where parents have chosen to save a child by giving birth to a younger sibling.
In 2001 a case in the United States caused controversy. A mother wanted to save her daughter who suffered from congenital Fanconi anemia. The mother used genetic screening to select a younger brother who would be suitable for umbilical cord blood transplants. Was this brother who was chosen to save his sister simply a "tool"? If he understood this reality when he grew up, would he bear doubts about the value of his existence? The conclusion that emerged from the public debate was that he wouldn't be harmed by giving his umbilical cord blood to his sister, and that the circumstances wouldn't diminish the love his parents had for him, so the uproar died down. But the remarkable impact of reproductive technology on people's lives was again noted.
"Human reproduction admits of choice," says Hsieh Fon-jou, who practices as an obstetrician at National Taiwan University Hospital (NTUH). He notes that before the 24th week an embryo lacks a heartbeat and isn't regarded as a person yet. Consequently, one method often used for those having trouble conceiving is to implant three or four fertilized eggs into the womb to increase the chances of at least one surviving. If several survive, the doctors then eliminate some. From the standpoint of the medical community, this action neither constitutes an abortion nor the killing of a life. Once a child is born, however, it is regarded as an independent and whole human being. Consequently, under the medical principle of "not giving up on any patient," prematurely born children with large numbers of complications cannot be given up on and left to die.
"When a life has already begun, society cannot withhold care," says Chang Tse-wen, a research fellow at the Academia Sinica's Genomics Research Center. The same principle is involved when National Health Insurance covers the provision of "orphan drugs" that benefit only a small number of patients. Society spends large amounts of medical resources on them. It may seem that this use of resources is unfair, but there is a side benefit: "Research into rare childhood diseases stimulates medical progress."
Be that as it may, the progress of medical technology in treating these rare diseases has been limited. Tseng Min-chieh, executive director of the Taiwan Foundation for Rare Disorders, points out that although about 3,000 people in Taiwan suffer from these disorders, only about 5% of them can be treated with orphan drugs; the remaining 95% receive no drugs. Because there are so few people with these rare but treatable disorders, the cost per person is staggering. All told, the nation spends about NT$1 billion on these drugs during an average year.
Children's medical rights
The argument goes that society has to take responsibility for these children's care once they are born. Yet, from another angle, the medical rights of Taiwan's children are being overlooked.
"Very few people in Taiwan are concerned about children's medical rights," says Lin Kai-hsin, a pediatric hematologist at NTUH. In dealing with parents from different socioeconomic backgrounds, doctors must find some means of communication to amply convey the methods and limits of medicine. But some things are hard to overcome: "When it comes to children people have lots of strange ideas, and sometimes parents' decisions are opposed to their doctor's judgment." Lin cites the blood disease thalassemia. Children who suffer from it and get blood transfusions and chelation therapy can lead normal lives. But some parents, wishing to avoid all this trouble, risk cord blood transplantation with poor genetic matches, and end up costing the children their lives. Lin feels at a loss and extremely frustrated every time he hears about one of these cases.
Before children come of age, they lack medical autonomy. Their parents or legal guardians must give consent if children are to participate in experiments or drug studies or to donate a liver or kidney. Sometimes moral pressure is exerted on the children. One teenage boy in Taiwan donated a piece of his liver to his father, and the decision was widely praised in society as an act of filial piety. But at the time the boy was conflicted. Did anyone respect his true feelings?
"In Taiwan the medical rights of children are clearly insufficient," says Liu Hung-en, an assistant professor of law at National Taipei University. He notes that relatives have almost complete rights to make decisions for children. Outsiders have very little say. In other countries, unreasonable medical decisions made by parents are regarded as child abuse, and charges can be filed by doctors or social workers.
Disease control vs. human rights
In the case of notifiable infectious diseases, human rights are wholly trampled upon for the sake of the general public good.
Because infectious diseases affect public safety, it is hard for disease prevention efforts not to come into to conflict with human rights. A painful example was the SARS outbreak in 2003, which caused 8000 infections and 744 deaths around the world.
In November 2007, a Taipei City committee charged with deciding how to spend funds donated to combat SARS, along with the Taipei City Department of Health, sponsored the 2007 International Symposium on Humane Care in the Post-SARS Era. At the symposium Dr. Robert G. Maunder of Toronto pointed out that during the outbreak, medical workers in Canada were first viewed as courageous heroes who risked death to perform their duties. Later, when growing numbers of medical workers contracted SARS, they became viewed as "spreaders of disease" and gradually came to be viewed in a bad light. One nurse who used public transit was chastised in the media for "irresponsibly disregarding public safety." Nurses treating SARS patients were forced to cancel their hairdressing sessions and their own doctor's appointments. Even these medical workers' children found themselves banned from various school activities.
Nowhere was the epidemic brought under control faster than in Vietnam (51 days), but it still led to quite a few human rights controversies there. Tham Dung Chi, a professor at Hanoi Medical University and acting chief of the National Institute of Hygiene and Epidemiology, explains that the Vietnamese armed forces took a forceful approach of putting disease prevention first. College students returning from Beijing, where many cases had occurred, were immediately brought into quarantine. This caused student protests. There were even bus drivers who abandoned their buses halfway through their routes for fear of catching the virus.
In Taiwan, the greatest controversy involved Taipei Municipal Hoping Hospital, which was suddenly sealed off without warning, and the identities of those with the disease were publicly revealed.
"By releasing the names of SARS patients to the media, who knows how much distress was caused to them!" remarks King Chwan-chuen, a professor in the Department of Public Health at NTU. In the face of a new disease, everyone is ignorant and panic stricken. But no matter what, you can't ignore human rights.
Lament of the innocent
When disease prevention is viewed like going to war, and you force medical personnel, who have no military training, to risk death by holding fort at a hospital where the disease is rampant, and then you take SARS patients and other patients, as well as doctors and nurses, and lump them all together, it is not only unlawful-it also violates basic human rights. From the extent of the victims' distress, you can see that the pain these decisions inflicted greatly exceeded the physical suffering and death caused by the disease itself.
About a year and half after the outbreak, Su Tung-ping, director of Taipei Veterans General Hospital, conducted a study on 107 medical workers who had contracted SARS and discovered that 73% of them went on to suffer from depression, 68% of them from post-traumatic stress syndrome, and 18% from panic disorder.
Beginning in 2004, Taipei began to implement a long-term care plan for SARS sufferers. Yang Tsui-yuang, director of the Songde branch of Taipei City Hospital, points out that of the 281 people who contracted SARS in Taipei City that year, only 145 were willing to participate. Of the remaining, 23 could not be traced, 13 had died, 29 refused to provide any data or accept any care, and 27 weren't even willing to talk.
"Sufferers not only get labeled and rejected; they also become subjects of research, have needles stuck in them for blood samples, and get asked to go to court and testify," explains Yang "There are cases where people have broken under the pressure and have ended up having to leave their jobs or getting divorced. It changes everything. People's suffering far exceeds the health impacts of the disease itself." Yang cites the chairman of a SARS support group as example. He used to run a small business, but after he had come down with SARS, not only did all of his workers quit, even his next-door neighbors would give him and his family members nasty looks. He was forced to move house, leave his career and start all over.
Medicine, not machine
"When a person is quarantined at home, there is a strong flavor of rejection," says Professor Yi-min Arthur Chen of National Yang-Ming University. During the SARS outbreak, 130,000 people in Taiwan were quarantined. Among these, 50,000 were subjected to Level-A quarantine (for SARS patients and those who had been in close contact with them); and 80,000 were subjected to Level-B quarantine (for those in areas where there were high numbers of patients, or those who had returned from travel to China, Hong Kong or Macao).
SARS brought with it separation and alienation, but it also made people reconsider how to go about reconciling public safety with respect for individuals' rights during outbreaks of disease.
Medicine and human rights have a complicated relationship that poses seemingly irresolvable difficulties. But if you leave the realm of science and law to look at matters from a philosophical vantage point, then the answers can seem quite simple.
"The universe is a huge idea, not a huge machine," says Hsieh Fon-jou. There may be no turning back on the advances of modern medical science and the implementation of various public health measures. But as we march down that road of progress, we should stop at times to take stock and reevaluate the purpose and meaning of our actions.







