What's Up, Doc?Taiwan's Medical Malaise
Chang Chiung-fang / photos Jimmy Lin / tr. by Phil Newell
April 2005

In the past two or three years, there have been a series of outrageous incidents involving medical negligence and malpractice. For example, at the North Town Women and Children's Hospital in Taipei County, muscle relaxants rather than vaccines were mistakenly injected into infants, causing the death of one newborn and side effects in several others. At Pingtung's Chung Ai Clinic, medicine to reduce blood sugar was wrongly given out as cold medication, causing a number of infants and children to lapse into a coma. At the Zhongxiao Branch of the Taipei City Hospital, medicine for athlete's foot was applied to patients suffering glaucoma. It is no surprise that citizens have been wondering about the quality of the health care they are getting.
Doubts about doctors' competence and even their basic morality turned to outright stupefaction during the incident in February of this year involving a young girl surnamed Chiu. After being beaten into unconsciousness by her own father, the child was subsequently refused admission to hospitals across Taipei, which all claimed they had already taking their quota of neurology patients. Like a bouncing ball, she was driven in an ambulance from hospital to hospital before finally being accepted at a hospital in Taichung City, a two-and-a-half-hour drive away from where she had suffered her injuries. She died in hospital.
Why are we seeing so many problems with Taiwan's health care system? What has gone wrong with doctor-patient relations? What can be done to remedy the defects?
Are doctor-patient relations getting worse?
Chang Ly-yun, chairman of the Taiwan Health Reform Foundation, believes that there never has been any golden age of doctor-patient relations. It is just that now the latent conflicts that have always existed are surfacing. "Doctor-patient relations haven't gotten worse; what we have now is a change in their nature."

The treatment of illness is a partnership between patient and doctor. Our photo shows Tsai Che-hsiung, vice-president of the Koo Foundation Sun Yat-sen Cancer Center, teaching students at the bedside.
Robin Hood no more?
With changes in the larger environment, health care has also inevitably changed.
Chiang Tung-liang, a professor at the Institute of Health Policy and Management of National Taiwan University (NTU), points out that the long-term penetration of capitalism into health management, plus the implementation of the National Health Insurance (NHI) program ten years ago, have certainly altered the relationship between physician and layman. In particular, since the NHI system was instituted, people's uncertainty about their ability to pay for treatment has largely disappeared. Doctors, who were formerly seen as "gourd-carrying saviors" (evoking the traditional image of ancient practitioners of Chinese medicine) or even as Robin Hoods helping the poor, have clearly lost a lot of status and respect. "Doctor-patient relations, like father-son relations, have been moving from an authoritarian era to one of partnership," Chiang concludes.
Over the last ten years the NHI system has come between doctor and patient, like an enormous barrier.
Chang Ly-yun relates that 30 or 40 years ago, doctors in local clinics were on very familiar terms with their patients. Even in hospitals, although the institutional intermediary of the hospital inserted itself into the doctor-patient relationship, doctors still enjoyed great autonomy and room to act as they saw fit. But today hospital administrators are increasingly powerful, and medical policy agencies in the government and the National Health Insurance Bureau (NHIB) are also involved, making things increasingly complex. The doctor-patient relationship no longer just involves a doctor and a patient, and is no longer simply a relationship between one human being and another.
Although the presence of a third party between the doctor and a patient-an institution that pays the bills-means that there is no direct conflict of interest between doctor and patient, physicians are still caught between "hospital costs" and "the best interests of the patient."
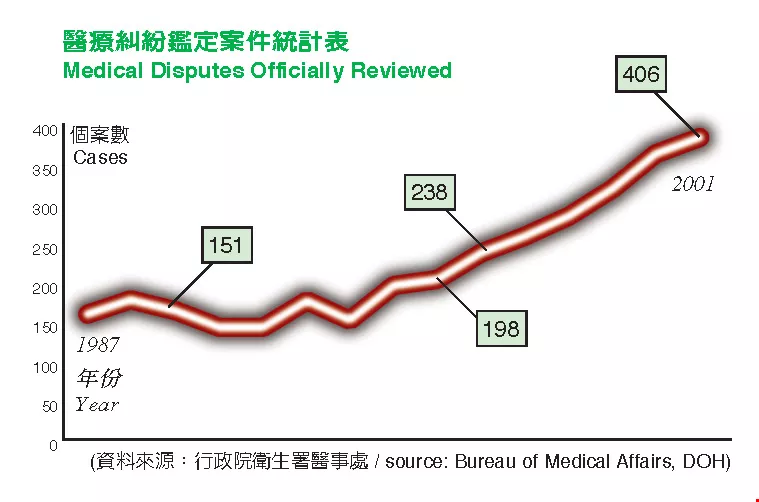
Medical Disputes Officially Reviewed source: Bureau of Medical Affairs, DOH
Misdirected attention
Besides the influence of the system as a whole, increasing reliance on technology has also widened the distance between doctor and patient.
After the incident involving the Chiu girl, Peng Hay-jan, an associate professor of social work and the dean of academic affairs at Tunghai University, was moved to analyze what has gone wrong. Hospitals today, he wrote, are vast, doctors are busy, and the administrative system is complex, so that even as hospitals hire more and more highly trained specialists and get better and better equipment, they lack "an atmosphere in which anyone bothers to think at all about how the patient feels."
Doctors have no empathy for how patients feel. Virtually everyone who has been to the hospital knows this feeling and how distressing it can be, even though many people find it hard to put into words.
According to a study by Michael Chung, an associate professor in the Graduate Institute of Health Care Organization Administration at NTU, when Taiwanese were asked what makes a good doctor, they responded: that she be caring and concerned about the patient (69.1%), that she clearly explain the medical situation (43.7%), and that she be highly skilled (37.2%). Clearly the human factors have top priority.
But today medical professionals place too much reliance on medical technology. They often give so much attention to the results of tests, medical histories, and numbers flashing on various instruments and devices that they ignore the fact that it is the patient, after all, who is being treated.
Ms. Chang, a bank employee in her thirties, knows the feeling first-hand. Before the Lunar New Year, she tested positive in a home pregnancy test. But when she went to a gynecologist for an examination, several ultrasounds failed to reveal any fetus. Suspecting it might be a case of extra-uterine pregnancy, the doctor-who looked like he must have been very experienced-blurted out right there in front of her, "Uh-oh, this looks really bad!" Ms. Chang was so frightened she burst out crying on the spot. She immediately switched to a different ob/gyn clinic.
The lack of empathy shown by many medical care providers is perhaps most acutely felt by emergency room patients.
A few days ago, a patient who had swallowed 30 or 40 Prozac was sent to the hospital. The first thing the emergency room physician said was, in a disdainful tone, "This isn't your first time, is it?" His voice betrayed his thoughts: "This guy is trouble. Why should I care about him?" Naturally this caused the patient even further humiliation. "Maybe medical people are dedicated to saving life, so they can't understand why anyone would want to destroy it," said this individual later, trying to see things from the doctor's point of view.

Their work is a matter of life and death, in which every second counts and they can't afford even the slightest mistake. The pressure on medical professionals can be immense.
Three longs and two shorts
Although at times doctor and patient are like a married couple enduring hard times hand in hand, in fact this partnership is increasingly short and shallow.
Perhaps the most widely complained-about aspect of medical culture in Taiwan is the "three longs and two shorts." There are long lines to register, long waits to actually get in to see the physician, and long waits to pick up prescriptions, while a patient only spends a short time with the doctor and the doctor keeps whatever explanations he gives very short.
According to a survey by the Taiwan Health Reform Foundation (THRF), published in 2002, nearly 65% of first-time patients and 53% of return patients spend less than five minutes with the doctor.
"This is a vicious cycle," says Andrew T. Huang, president of the Koo Foundation Sun Yat-sen Cancer Center (SYSCC), the nation's most prestigious institution in the field of oncology. Because doctors see so many patients, they can't spend more than a few minutes with each one. This raises the rate of misdiagnosis, so that patients lose faith in any single opinion. To protect themselves, they visit several doctors each time they feel out of sync. This increases the total number of patient visits, so that doctors have to make each consultation even shorter.
According to statistics from the NHIB, on average each Taiwanese visits the doctor 15.5 times per year. The average in OECD countries, in contrast, is 7.8, while in Europe and the US it ranges from four to seven times.
Andrew Huang relates that when Harvard University vice-president Harvey Fineberg was invited to Taiwan in 2001, and heard that it is the norm for a doctor here to see 100 patients in one shift, his immediate reaction was: "Ninety percent surely don't even need to be seeing a doctor!"
The pursuit of operational efficiency in medical practice thus gives rise to even greater inefficiency. Put more succinctly, haste makes waste.
"A doctor can't possibly diagnose a patient effectively in only two or three minutes," says Huang. Pointing to diabetes patients as a case in point, he says that a thorough check up, from under the eyelids to the peripheral nerves, takes at least 30 or 40 minutes. Any doctor who is getting his patient out the door after only two or three minutes is not solving the patient's problem at all, but is simply passing it along to the next guy in line. This kind of "treatment" is wasted effort for all concerned. "The medical industry is not just some ordinary consumer industry," Huang concludes. "The most 'efficient' visits are the ones that produce solutions."

Medical Disputes Officially Reviewed source: Bureau of Medical Affairs, DOH
Family value
So are we saying that hospitals shouldn't seek to be efficient?
Chang Ly-yun replies in part by saying that the idea that many people have that hospitals are not money-making institutions, and should therefore not seek efficiency and profit, is not correct. Medical resources are limited, so efficiency in use is a legitimate goal. What her group, the THRF, sees as most unfair is not cost-cutting per se, but the fact that in reducing expenses hospitals simply pass on many of the costs to society as a whole.
The best example of this is the shortage of nursing staff. Chang queries, "These days, who dares to leave their relatives in the hospital without some family members to be with them?" In order to save on manpower, she says, hospitals don't hire enough nurses, leaving family members to pick up the slack. It is quite common to see a situation in which "when one person gets sick, the whole family stays in the hospital." Even during the SARS epidemic, when relatives and even nursing staff were forbidden to have direct contact with infectious patients, and hospitals were considered high-risk zones, people who had no business being there could be seen wandering in and out.
When Ms. Wang gave birth by Caesarean section, her baby daughter had to remain in hospital because she had inhaled some amniotic fluid into her lungs during birth. While recovering from the delivery and still in the hospital herself, Ms. Wang repeatedly asked to see the doctor in charge of her baby's case. But the response she got was invariably: "The doctor is very busy and has no time." Right up to the time she was discharged from the hospital, she never even got to see the doctor's face.
Little did she expect that almost as soon as she left the hospital and returned home, she would get a phone call telling her to return to the hospital to hold her baby for an x-ray. She was flabbergasted: Wasn't her child being looked after in the hospital? Weren't there nurses who could carry the child down to radiology? The answer she got was, "None of the nurses here has ever had kids, so who's going to be able to hold the baby for you?" Ms. Wang had no choice but to phone her husband at work and tell him to take a run over to the hospital. Incredibly, hardly had Dad left than hospital than they called again, telling Ms. Wang they needed to take another x-ray. The reason was that they had made mistake on the first one, taking a film of the right instead of the left lung. "I wanted to scream. That's what our hospitals call 'quality care,'" she says, clearly galled by the whole experience.

Healing the body and the mind-under the diligent care of doctors, patients gain the courage and strength of spirit to fight off their illnesses. This photo shows a scene from Taiwan Medical University's affiliated hospital.
Failure to communicate
Medicine is a skill, but it is also an art.
Raanan Gillon, a medical ethicist from the UK, has said that doctors today not only need to be skilled in the practice of medicine, they must also be excellent communicators. Only if they communicate well can needless medical disputes be avoided.
In fact, most cases of misdiagnosis or malpractice arise from failure to communicate. Given doctors' heavy reliance on medical jargon, the short times permitted for consultations, and the "infantilization" of patients by medicos, it is no surprise that patients and physicians end up talking right past one another.
According to statistics from the Department of Health, the number of disputes over medical treatment in Taiwan has doubled in the past ten years, to reach almost one per day. On average, out of every five cases that are formally opened, there is one case in which the verdict is malpractice.
Medical malpractice can have a dramatic impact on the public. Each year in the US, between 44,000 and 98,000 people die as a result of medical negligence and error, making this the eighth leading cause of death.
In a 2002 master's thesis for the Graduate Institute of Health Care Organization Administration at NTU entitled "The Physician's Knowledge, Attitude, and Response toward Patient Safety Issues," Chang Pi-cheng found that 30.6% of doctors in northern Taiwan had committed errors in medical practice. The most common error was incorrect evaluation (25.4%), with the main cause being lack of experience (also 25.4%). Of these mistakes, 70% had effects on the patients, including longer hospital stays (41.7%), extra treatment or therapy (39.3%), and even, in 17.46% of incidents, death.
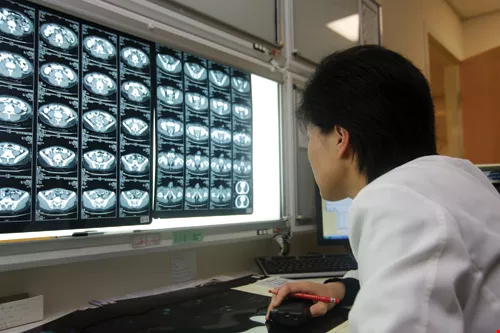
As technology has progressed, all kinds of instruments have been developed that theoretically help doctors make more accurate diagnoses, but this may have also led to their neglecting the most essential element of medicine-the people.
Doctors, not deities
"If doctors and patients could each take one step toward the other, and engage in a little more meaningful dialogue, not only would this reduce waste of medical resources, it could avoid many disputes over treatment," says Chang Ly-yun.
A man surnamed Hsiao relates that once when he was waiting to see the doctor he saw pamphlets printed by the THRF entitled "Think Twice and Ask Three Times before Surgery." He picked one up, and followed its instructions to engage in a dialogue with the doctor. The result of their extensive discussion was that he discovered that he only needed continued observation, not surgery. He felt like he had dodged a bullet.
Chu Tung-kuang, deputy director-general of the Bureau of Medical Affairs in the Department of Health, says that people being complex organisms, there are significant differences between individuals, so medicine has by nature a high degree of uncertainty. It's sometimes very difficult to say that a doctor has made a mistake-sometimes it is simply that doctors and patients come away with very different ideas in their heads, and patients "cannot emotionally accept the results of their consultations or treatment."
We can see something of this dilemma by looking at a few cases that have made it into the courts.
Five years ago in Keelung, a neurosurgeon named Chen was found guilty of professional negligence leading to the death of a patient. The incident began when a man named Lin, who had been sent to the hospital with a depressed fracture of the posterior cranial fossa (the rear part of the base of the skull) resulting from a traffic accident, died unexpectedly from complications related to the injury. His family members then sued the doctor.
Complications resulting from injuries to the posterior cranial fossa are not very easy to discover, because right up until the time they become life-threatening, the only symptoms are headache, dizziness, and other non-specific neurological symptoms. Thus it is by no means always easy to tell when complications are setting in. But when the complications become severe, for example, if cerebral edema (swelling of the brain) presses down on the brain stem, and timely action is not taken to control the situation, the result can be sudden death at any moment.
The case was twice analyzed by the medical review board, which, despite having many different views about what would have been the most appropriate course for the doctor to take, each time indicated: "based on the patient's medical history, the x-rays, and the computerized tomography (CT) scan, it was not absolutely impossible to discover that the patient was suffering from increasingly severe cerebral edema." Relying on this conclusion, the judge decided there must have been shortcomings in the treatment which made timely action to save the patient impossible. But on the other hand, taking into account the doctor's previous good record, the fact that neurosurgery is by definition a high-risk field, and the fact that the specific complications in the case are rare, the judge recommended "lenient punishment."
The moral of the story is that doctors are not miracle workers. Indeed, medicine as a science is relatively in its infancy. It was only in the early 1940s, with the discovery of antibiotics, that doctors began to change their role from passive care-giving to active therapy. But although there are things doctors can do, this does not mean that they can do everything.
At a medical ethics conference entitled "When Patient Meets Doctor," Hsu Cho-yun, a fellow of Academia Sinica and a self-proclaimed "veteran patient" (being a victim of polio since childhood), related that he is well aware, based on his own experience, that all treatments and therapies have their limitations. Therefore, he advised, doctors should let patients know that "the science of medicine is not completely scientific." They should make the most sincere effort they can, so that even if the treatment does not yield the anticipated results, the patient will be able to understand and forgive.
However, looking at things from the other side, if you want people to understand and forgive, then the medical industry should make much more information of all types available to the public, so that people have the means to understand and the bases on which to make informed choices.
"The health-care industry is an industry of asymmetrical information," says public health professor Michael Chung. In the jargon of medical economics, the health-care industry is an "imperfectly competitive market." It is impossible to see into the "black boxes" in which hospitals and doctors make choices, so it is difficult to judge whether they have acted properly or not. Hospitals make their own evaluations, of course, but these are done behind closed doors, with the medical community sitting in judgment on itself; outsiders are completely excluded from the process.

Providing education on health and hygiene to raise the level of awareness in the community is a way of knocking down obstacles to good communication between doctors and patients, and is a hospital's duty. This photo shows the service area at Taipei Medical University's affiliated hospital.
Friends, not enemies
The asymmetry between patient and doctor is not only a question of information transparency, it is also a problem of basic knowledge and understanding.
The non-governmental Taiwan Health Reform Foundation was founded in 2000 to help out on the patients' side of this (im)balance, to create an opportunity for dialogue between doctors and patients.
Over the past four years, the THRF has played the role of "whistle blower," drawing attention to many problems. Though some medical professionals consider the foundation a "plague," and say that it is just a bunch of outsiders criticizing something they don't understand, THRF chairwoman Chang Ly-yun, a sociologist by training, replies, "If we were trying to treat patients, of course we would be outsiders, but who can possibly remain outside of health care as a public matter?" The foundation simply seeks to smash the arrogance and absurdity of those in the medical community who think, "if you don't understand the science, you have no right to have an opinion on the health care system."
"It is simply that THRF has adopted a perspective that is different from that of doctors, but we are not opposing ourselves to them!" This sentence, it seems, could apply equally well to the relations between doctors and patients. Chang believes that the best way to improve the quality of health care in Taiwan is to let patients participate more. This will also become one link in the chain of preventive medicine.
"The purpose of providing patients with basic treatment information, such as labels on prescription medicines, access to their own medical histories, and agreement forms for surgery, is to allow patients to understand what doctors are doing. Because if by chance the doctors or nurses make a mistake, this is the only way the patient will have a chance to find out what really happened." Chang emphasizes that this "empowerment" of patients is not a challenge to or attempt to seize authority, but is a measure to prevent the occurrence of even more serious medical mistakes.
However, coordination, participation, and discussion require an accommodating environment. "How many hospitals have the time or space to let doctors and patients really talk?" queries Chang.
In recent years doctors have been encouraging patients faced with major decisions to seek "a second opinion." But in practice this is very difficult. The main obstacle is acquisition of medical records.
Chang Ly-yun points out that few ordinary people have the tools to accurately describe their conditions; they need help from test results and patient histories. But patients who want to access their own records now have to tell a lie-it is almost impossible to succeed unless they are requesting the records "on behalf of the insurance provider."
"If we could follow the American model, in which hospitals have a duty to provide medical records to patients, then we wouldn't need to put the burden on the patients. What's more, when a medical professional knows that what they write on the charts is going to perhaps be reviewed by one of their peers, they will be more careful and precise in what they write."
On top of medical records, in the future the THRF will propose the creation of "pharmaceutical records." Chang says that if a patient has to visit several departments, there can sometimes be duplication of prescriptions, or even prescribing of drugs that will, taken together, have severe side effects. If each patient has a "pharmaceutical record" to carry around, doctors in different departments can take into account what other doctors have decided, and make the necessary adjustments.
Soft revolution
In contrast to the more abrasive approach of the THRF, Michael Chung is more inclined to a "gentle revolution" based on self reflection and learning in the medical community itself. "After all, we still need doctors-don't scare them off!"
As accusations and criticisms criss-cross back and forth, some in the medical profession believe it is necessary to step back and gain some perspective on the issues.
Li Yuan-te, former head of National Taiwan University Hospital and now a professor at NTU's College of Medicine, has pointed out in a published article that a German magazine on family medicine has praised Taiwan as being "an exemplary model despite being kept outside the WHO," the ABC television network in the US has called Taiwan "a health utopia," and health care services in Taiwan are ranked second among OECD countries. "Each day in Taiwan there are 780,000 medical consultations," says Li, "and each year there are 2.88 million hospital stays. Isn't it being much too negative just to pick out the 200 medical disputes and thereby obscure the vast contributions made by the medical profession?"
A patient-doctor treaty
Be that as it may, it is also true that in recent years even many members of the medical community have begun to reflect on the problems in the system.
For example, there have been efforts to clarify in both theory and nomenclature the relationship between doctors and patients. Whereas Taiwanese have always used the expression "doctor-patient relations," these days there is a quiet shift to the term "patient-doctor relations."
"The patient-doctor relationship is a very intimate relationship," says Andrew Huang of the SYSCC, who returned to Taiwan 16 years ago. To construct an intimate relationship of this nature, "doctors have to lead the way by being the first to change."
In July 2003 at a conference on health care in the wake of SARS, Huang began to promote the idea of a patient-doctor alliance, complete with a "patient-doctor agreement." Such an agreement would read, in part, "As doctors, to whom patients entrust their lives, we will do all we can to relieve the patient's pain, and contribute all we can to promote the health of the patient. We will listen carefully to the patient's complaints, inquire in detail to get the complete medical history, and use caution in undertaking essential tests and procedures, and will also exchange views with other doctors.... We will leave no stone unturned to explain to each patient his or her medical condition, to respond to questions, and to resolve doubts, and we will aim to help each patient gain complete understanding.... We will not accept grants or profit shares from hospitals, pharmaceuticals manufacturers, or other businesses, which would require us to use specific methods to treat patients.... We believe that the dignity of the medical profession and the trust of the public come from our own commitment as doctors to keep in mind and to put into practice our professional oaths."
As written, this proposed "patient-doctor agreement" imposes demands and rules only on physicians, and inevitably many people have condemned it as mere "hot air." Although it does sound filled with platitudes and is very ambitious, Andrew Huang and others like him not only believe that it can be applied in practice, they have begun to promote it in hospitals and through the education system.
We look forward to the day when the patient-doctor agreement will spread to all hospitals, when doctors can really keep their oaths constantly in mind. Perhaps in this age when health insurance, hospital administrators, high technology, and other "third parties" have come between patients and doctors, upholding the basic mutuality of the relationship between patient and doctor-between, at the most basic level, two human beings-we can help remedy the shortcomings in our medical system.
That will be the day when Taiwan can truly be considered a "medical utopia."
Questions for consideration
Do I need surgery?
Why do I need surgery?
What will happen if I don't get surgery?
Are any other treatment options available?
What kind of surgery do I need?
Which type of surgical procedure do I need? What are the possible complications?
Which type of anesthetic will I need? Does the hospital have a professional anesthetist available to oversee the whole procedure?
Who will do the operation? How skilled a surgeon is he/she?
After the surgery, what's next?
How long will it take for me to return to full health after the operation?
Do I have any more doubts or questions about the surgery?
(courtesy of the Taiwan Health Reform Foundation, compiled by Chang Chiung-fang)



@List.jpg?w=522&h=410&mode=crop&format=webp&quality=80)



