Return of the White Plague?--The Tuberculosis Control Effort
Chang Chiung-fang / photos Chuang Kung-ju / tr. by Minn Song
December 2003

During these days of brilliant au-tumn sunshine and mild breezes, many people still recall the battle with SARS that began in the fall of last year. That struggle provided a vivid lesson in the formidable might of disease to a public that had been long negligent about preventive measures.
In fact, the threat to humanity posed by disease has never been far off. Besides the continual appearance of previously unseen infectious diseases such as SARS that catch people off guard, others that have been with humanity since ancient times still torment us. They wait for an opportunity, and just when people seem to have forgotten these old foes' existence, they strike again. Tuberculosis (TB) is just such a disease.
"Every 36 minutes, there is a new tuberculosis patient, and every six hours another person dies of tuberculosis." These alarming figures describe the present situation in Taiwan.
TB has long been the deadliest infectious disease in Taiwan. For example, last year more than 1,200 people died of tuberculosis, and in some areas, such as Kaohsiung City, Keelung City, Changhua County, and Taitung County, TB even ranked among the ten most common causes of death. Tuberculosis is the biggest killer among infectious diseases, and is more fearsome than enteritis, dengue fever, AIDS, and SARS combined-at least in terms of the total number of deaths caused.
TB is no less serious than SARS, yet annual expenditures in Taiwan for tuberculosis prevention amount to only something over NT$100 million. Compare this figure to the NT$50 billion budget appropriated in one fell swoop for SARS prevention, and the enormous disparity is apparent. In fighting tuberculosis, what are Taiwan's prospects for success? This is a question deserving consideration.
As the SARS epidemic began to wane in early May, there came the startling news of an outbreak of TB at a Taipei hospital. At the end of August, a small outbreak of infectious tuberculosis was reported at Hualien Hospital. After extensive investigation, though 31 of more than 1,000 employees tested at the Taipei hospital showed abnormalities in their chest X-rays, it was still difficult to ascertain whether the source of infection was transmission among people within the hospital. The incident at the Hualien Hospital turned out to be a false alarm.
After the "baptism of fire" provided by SARS, health care facilities began casting the same suspicious eye they had on potential SARS victims on possible victims of tuberculosis, which like SARS is an infectious disease that afflicts the respiratory tract. As a result, the level of caution and worry about outbreaks inside hospitals also increased.
While SARS was prevalent, the increase in stress and the resultant weakening of immune functions enabled TB to spread and develop into active cases easily. Victims who were afraid to go to hospitals to obtain medicine or who had no one to supervise the taking of medication may also have caused increases in the number the failed treatments and the incidence of drug-resistant bacterial strains. However, SARS did at least have one salutary effect-it called the medical profession's attention to tuberculosis.
Though TB does not strike as abruptly as SARS, the enormous impact that SARS had on Taiwan's infectious disease prevention efforts has made the Department of Health's Center for Disease Control (CDC) anxious to build up the weaker links in the tuberculosis prevention regime. Therefore, at the end of August it organized a "Conference on Tuberculosis Prevention in the Post-SARS Era," gathering together experts from healthcare, academic, and public health circles, in the hope of increasing awareness and preparedness.
Wu Yi-chun, head of the TB division at the CDC, asserts that TB is less of a threat than SARS. Though both diseases have the same route of transmission-infection by airborne droplets-SARS is caused by a new pathogen, and the entire public lacks antibodies to it, while M. tuberculosis is a very ancient bacterium. TB is not highly contagious, and even if a person is infected, treatment can effect a complete cure. There is no need for panic.
Still, the cruel fact set before us is that roughly 1,200 people in Taiwan die every year of tuberculosis-more than from any other infectious disease. Compared to other countries with modern health care systems, Taiwan still has a rather high fatality rate from TB. The vestiges of the "sick man of Asia" label still remain.
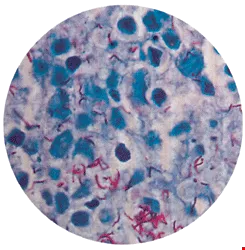
Mycobacterium tuberculosis. (courtesy of the Center for Disease Control, DOH)
An ancient disease has never left us
Called the "white plague" in Chinese, tuberculosis is an ancient infectious disease that has existed for a long time. From diseased tissues in the skeletal remains of people from the Neolithic age and ancient mummies, scientists have discovered that even in prehistoric times, human beings contracted tuberculosis.
The earliest recorded mention of tuberculosis in China is in the early Han period's Canon of Medicine, where the disease was called xu-lao. Writings of the time made frequent mention of this disease, with most reflecting a belief that pulmonary tuberculosis was caused by an insect wreaking havoc within the lungs. In The Mad Monk, when the Duke of Qi treated persons with tuberculosis, he would mutter, "Pest, pest, with your form like a bee, you burrow into the bone marrow, devouring blood. The victim cannot be saved, and the physician knows not how to attack."
In The Dream of the Red Chamber, Lin Daiyu often writhed in bed, coughing incessantly, in the end coughing up blood and expiring-apparently the classic symptoms of tuberculosis.
In the eighteenth and nineteenth centuries, Europe experienced tuberculosis epidemics, but the cause of the disease remained unclear at the time. It was not until 1882 that German physician Robert Koch discovered the cause of tuberculosis-Mycobacterium tuberculosis-and that the misconception that tuberculosis was due to a genetic predisposition was put to rest. The disease was from then on classified as an infectious disease caused by a bacterium.
However, the discovery of the disease's cause did not provide the means to treat it. Effective anti-tuberculosis drugs did not emerge until 1950, and during the preceding 100 years or so, it is estimated that TB claimed 200 million lives around the world.
Before the discovery of effective anti-tuberculosis drugs, physicians used surgical excision of pulmonary lobes or passive therapeutic measures to fight TB. It was only when drugs such as streptomycin and para-aminosalicylate were successively found able to effectively treat tuberculosis that humanity could be said to have escaped the curse of the "white plague" In the 1970s, the new drug rifampicin (RFP) was successfully developed, reducing the treatment regimen for TB from two years to half a year. TB was no longer a terminal illness.
Regrettably, though effective treatments had been found, this did not lead to the disease's elimination. On the contrary, in the late 1980s the incidence of active tuberculosis cases and the mortality rate began to rise once more. The appearance of drug-resistant forms of M. tuberculosis has increased the difficulty of treating tuberculosis.
According to WHO estimates, at present one out of every three people in the world has already been infected by the TB bacillus and each year as many as 8 million people develop active TB. Medecins Sans Frontieres (Doctors Without Borders) also warns that in the next ten years, 30 million people may die of TB. At that point, this infectious disease, which was once considered under effective control, will become humanity's biggest killer. The WHO therefore urges that the world once again pay attention to the prevention, diagnosis and treatment of tuberculosis.

Taipei's Hospital for Chronic Diseases is the only remaining hospital specializing in tuberculosis treatment.Hospital director Joz Lu is shown examining a parient.
Early discovery, early treatment?
Why has tuberculosis been so difficult to eliminate?
For any disease, early detection and early treatment are the most effective control measures. But for TB, achieving a correct diagnosis early in the course of the disease and a subsequent complete treatment regimen both present challenges.
Discovered a hundred years ago, the Bacillus Calmette-Guerin (BCG) vaccine is still used to prevent TB. In Taiwan, excepting infants with genetic diseases or those born prematurely, 98% of newborns are given a BCG vaccination in order to prevent tubercular meningitis.
However, the vaccine remains effective for only ten years, and provides no immunity in adults. In other words, once past the period during which the BCG vaccine can provide protection, everyone runs the risk of infection and of contracting TB.
Interestingly, statistics reveal that tuberculosis afflicts males and females unequally, with males three times more likely to contract the disease. Suo Jen, a tuberculosis specialist at Taoyuan General Hospital, points out that before the age of 35, the disparity between males and females is not great. But with advancing age, the difference becomes increasingly evident, and by age 67, the ratio of male to female victims reaches three to one. Some surmise that the disparity is related to hormonal effects, but as yet no firm conclusions have been reached.
Furthermore, due to factors such as the presence of other chronic illnesses and weakened overall resistance to disease, the elderly are the group with the highest incidence of TB. Currently, of the 19,000 reported suspected cases of tuberculosis in Taiwan, 46% are among persons aged 65 or older.
More unusually, Taiwanese Aborigines are also a high-risk group for tuberculosis. Though they are home to only 1% of Taiwan's total population, the mountain villages largely inhabited by Aborigines account for 3 to 5% of all reported cases of TB. According to statistics, the incidence of tuberculosis in mountain villages is four times higher than in the plains, while the mortality rate is six times greater. Suo believes that the high incidence and mortality of TB in mountain villages may be related to such factors as Aborigines' economic status, education, environment, lifestyles, personal hygiene, and willingness to seek and comply with medical advice.
Although TB is an ancient disease, the factors influencing its pathological course remain unknown. In other words, it is still a mystery why some people develop active cases after infection, while others do not. However, when a person is infected by the TB bacillus, he will not usually immediately develop full-blown tuberculosis, and the bacterium may remain latent inside the body for a long period of time. Generally speaking, once infected, there is a roughly 10% chance of a person developing an active case during the rest of his life. Of those who do develop TB, half do so within five years of infection. Once the full-blown disease emerges, if the condition goes untreated, one out of two people will die within five years. Another quarter of such patients will see their TB go into remission, a state where it is no longer active, though it may reemerge at any time. In addition, in one out of four patients, the disease becomes chronic and the person may continue to infect other people.
As far as we know, of those persons who are in close contact with an infectious tuberculosis patient-such as family members and co-workers-roughly one in three will become infected. A patient with an active case of tuberculosis can on average infect ten to 15 healthy people per year with the TB bacillus.
Due to the long latency period, early detection of TB is very difficult. And even if a patient already exhibits some minor signs of the disease, a correct diagnosis is also not easy.
A chest X-ray and sputum tests are the current methods for establishing a tuberculosis diagnosis. However, these two methods both have their blind spots. Chest X-rays will not necessarily be able to accurately capture lesions, as the lungs have five lobes, and there are more than 100 different types of bacillus that commonly infect the lungs. Moreover, tests of sputum will not always reliably detect M. tuberculosis. Under these circumstances, a physician's experience and professional training are extremely important.
Statistics show that two or three months typically elapse between the time a TB victim first shows symptoms and when he seeks medical assistance. Then from that time until a diagnosis is confirmed and treatment begins, another two or three months usually pass. In other words, from the time a tuberculosis victim first shows symptoms of the disease and the time when treatment begins, an average of half of year will have gone by. This lengthy period provides a window of opportunity for further infection that is very difficult to control.
After discovering tuberculosis, comprehensive treatment is yet another challenge.
Tuberculosis is not an untreatable illness. Generally speaking, if only medication is taken properly for two weeks, the patient will no longer be infectious, and continuing this course for six to nine months will effect a cure.
Patients with active tuberculosis must be quarantined and given treatment in a hospital until the infectious period is over. At present, there is only one hospital specializing in tuberculosis in all of Taiwan-Taipei's Hospital for Chronic Diseases, which maintains 17 negative-pressure isolation rooms used specifically for patients with active TB.
After the first phase of treatment is completed, and it has been confirmed that the patient's sputum is pathogen-free, the patient can be allowed to leave the hospital. After being discharged, patients must continue to take medication for six to nine months. Because they must swallow six or seven pills every day over a long period-with some patients developing side effects such as liver damage and loss of appetite-patients often cannot tolerate the drug treatment and quit before completing the full course of medication.
If treatment cannot be completed, it will result in a very serious consequence-the creation of drug-resistant bacterial strains, which are a thorny problem for current efforts to control pulmonary tuberculosis. Joz Lu, director of Taipei's Hospital for Chronic Diseases, points out that once the M. tuberculosis in a patient's body develops drug resistance, his tuberculosis becomes both chronic and active. Not only will such a patient's own illness be extremely difficult to treat, but if the drug-resistant bacterial strain harbored by the patient's body infects other people, they too will become carriers and victims of the same intractable form of tuberculosis.
Tuberculosis prevention postage stamps issued by the National Tuberculosis Association. Such stamps were used both to raise funds for tuberculosis prevention efforts and to raise public awareness. (courtesy of the National Tuberculosis Association)
The TB prevention network
Difficult to detect in its early stages, and requiring long periods of treatment, TB is not only difficult to eradicate, but is even becoming more prevalent. Faced with this stubborn disease, the establishment of a disease prevention regime is critical. Taiwan's achievements in this area in earlier years were worthy of pride.
With the support and assistance of the WHO, Taiwan gradually built up a rigorous tuberculosis prevention regime and aggressive patient management system beginning in 1955.
In the 1970s, besides Taipei's and Kaohsiung's establishment of their own tuberculosis control offices, the Taiwan Provincial Government's Tuberculosis Prevention Bureau coordinated the operations of the local tuberculosis control bureaus and offices in the 22 counties and cities under its jurisdiction. The result was the establishment of a comprehensive tuberculosis prevention network encompassing institutions from the Tuberculosis Prevention Bureau and the Institute of Tuberculosis Control, to the tuberculosis prevention workers stationed in local public health centers.
Mobile X-ray labs provided free examinations from the mountains down to the coasts, and were a familiar sight in Taiwan's towns and villages in those days. The National Tuberculosis Association issued tuberculosis prevention postage stamps, using the education system to raise funds, and at all times reminded the public of the importance of tuberculosis prevention. These campaigns are part of the collective memory of Taiwanese who grew up in the 1950s and 1960s.
Suo Jen of the Taoyuan General Hospital points out that with all-out mobilization and broad public awareness, the results of Taiwan's tuberculosis prevention efforts were excellent. In 1985, the ranking of tuberculosis as a cause of death fell out of the top ten for the first time. In 1986, deaths from tuberculosis for the first time declined to less than ten per 100,000.
Then, as tuberculosis prevention had already achieved its intermediate objectives, and as other chronic diseases were increasing in prevalence, tuberculosis hospitals began concurrently providing care for other chronic illnesses. In 1989, the TB control system was officially transformed into a chronic disease control system.
In 1995, with the introduction of the National Health Insurance (NHI) program, the public's habits in seeking medical care also changed. Tuberculosis patients, who had previously sought treatment at specialized hospitals, would now go to a nearby regular hospital. According to statistics, the rate at which TB patients sought medical assistance at regular hospitals increased from something over 20% to more than 70% in the first two years after the implementation of the NHI program.
Suo points out that city and county TB control offices experienced a gradual reduction in their range of functions and their overall scale. In addition, in 1999, after the streamlining of the provincial government, city and county chronic disease control offices either were merged with other agencies or discontinued their tuberculosis operations. Medical care for TB gradually shifted from specialist hospitals to regular health care institutions. Some of the highly trained tuberculosis specialists retired, while others left their jobs, or were assigned to other positions. The old TB prevention infrastructure today no longer exists.
With the dismantling of the old system, and a new regime as yet incomplete, correct diagnosis and patient tracking have become two large gaps in Taiwan's current TB prevention network.
After responsibility for the diagnosis and treatment of TB expanded from specialized hospitals to regular medical institutions, because of the latter's lack of opportunities to deal with TB victims, it is difficult for their physicians to discern from coloration, density, and irregular shadows in chest X-rays whether or not a patient has TB (to correctly read an X-ray for pulmonary tuberculosis requires at least a half to one year of experience). In addition, more than 85% of community hospitals and more than half of regional hospitals lack the facilities and personnel for culture labs, and therefore do not perform M. tuberculosis culturing. Five-sixths of all hospitals do not provide a "sputum collection room" where patients can cough up sputum, or they simply avoid the bother of collecting samples, and so do not test patients' sputum. These various factors have caused a marked decline in the rate of accurate TB diagnosis.
Suo points out that in recent years, the proportion of reported TB cases that have been changed from "suspected" to "confirmed negative" has increased from 10% to 20%. Some patients are blindly given medication even though it is unclear whether they in fact have contracted tuberculosis. Other patients, unable to obtain specialized medical care, spread M. tuberculosis while wandering from one regular health care institution to another.
In order to strengthen the tuberculosis treatment network, the Department of Health has made preliminary plans to use Taipei's Hospital for Chronic Diseases, Taoyuan Hospital, Taichung Hospital, the Center for Chest Disease, and Buddhist Tzu Chi General Hospital as diagnostic referral centers for northern, central, and southern Taiwan, accepting TB patients who have been diagnosed at regular hospitals or whose disease is proving difficult to treat.
These plans are being undertaken because regular health care institutions do not have the resources to manage tuberculosis patients, creating another gap in the tuberculosis prevention regime. Wu Yi-chun, head of the TB control division at the Center for Disease Control, admits that the weakest element in current TB prevention efforts is patient management. She points out that the CDC is currently in discussions with the Bureau of National Health Insurance, hoping to be able to shift to a care-quality-based system for calculating compensation given to hospitals to cover patient management costs. In order to increase the effectiveness of case management, the CDC will also select particular regions for a small-scale implementation of a standard Directly Observed Treatment, Short-Course (DOTS) program.
Tuberculosis prevention postage stamps issued by the National Tuberculosis Association. Such stamps were used both to raise funds for tuberculosis prevention efforts and to raise public awareness. (courtesy of the National Tuberculosis Association)
Retrieving lost sheep-DOTS
The DOTS program is a short-term direct observation and treatment program promoted by the WHO to deal with the problem of patients not taking their medication. This approach emphasizes a principle of "one person gets sick, two people get concerned"-meaning that one observer and one local nurse will each day monitor a patient to make sure that he takes his medication.
Each year in Taiwan there are roughly 14,000 to 15,000 new cases of tuberculosis, with a cure rate of 74.2%, a mortality rate of 18.3%, and "lost" cases amounting to 7%. These "lost sheep," the 7% of tuberculosis victims of whom the authorities lose track, are likely to cause the emergence of drug-resistant bacterial strains, increasing the difficulty of treating TB and raising the infection rate.
In fact, in 1997 Taiwan began implementing a small-scale tuberculosis DOTS program, with the focus placed on mountain villages with high incidences of TB. However, because of the widely dispersed population in such villages and insufficient personnel, there has not been comprehensive implementation of the program. According to a field survey of mountain villages conducted by Chou Chih-Chien, director of nursing at Taipei's Hospital for Chronic Diseases, 45% of victims do not know of the DOTS program, and 40% lack anyone to ensure that they are indeed taking their medication. Compared to the implementation standard utilized in mainland China-which requires that observers confirm that the medication is placed in the patient's hand, is put in the mouth, and then is swallowed before he is allowed to leave-Taiwan's efforts still need to be strengthened.
Taipei's Hospital for Chronic Diseases is targeting its DOTS program at older persons who are alcohol abusers, drug users, homeless, or who lack a social support system. You Chiu-chen, head nurse at the hospital, indicates that from 1997 to the present, 100% of the 50 cases in which there has been actual direct supervision have resulted in a complete cure.
You points out that the tracking of the homeless, who have no fixed address, and recruitment of volunteers to serve as DOTS monitors, are two major difficulties. To deal with the former, boxed meals or spending money are provided as an incentive, while reimbursement of travel expenses is used to compensate volunteers. She indicates that because TB is an infectious disease, due to safety considerations neither the Social Affairs Bureau's resident caregivers nor staff from private-sector charitable organizations are willing to serve as volunteer monitors. Because of the difficulty in locating monitors, at present most tuberculosis victims in Taipei have family members as their monitors, with the public health nurse periodically checking whether the medication is being administered correctly by a home visit or over the phone.

Besides regular screening conducted at schools of all levels, mobile X-ray labs also provide free, periodic tuberculosis screening in rural communities.
Destigmatizing TB-the DOTS Club
In recent years, Taiwan's death rate from tuberculosis has risen over three per 100,000, substantially higher than the two per 100,000 in other advanced countries. Joz Lu points out that the TB pathogen thrives in damp island environments. Moreover, factors such as Taiwanese citizens' long-standing stigmatization of tuberculosis, which leads to a reluctance to seek medical assistance, and poor habits in taking medication, have also led to a relatively high TB death rate.
While tuberculosis remains stigmatized, in order to protect the privacy of tuberculosis victims, and out of the concern that once their illness is revealed victims may be ostracized in the workplace, disease control authorities cannot and will not directly perform screening at a victim's place of employment. You Chiu-chen points out that at present all that can be done is to drive mobile X-ray labs to the vicinity of the workplace, and circuitously invite coworkers to get tested.
In order to overcome citizens' stereotypes about tuberculosis, Taipei's Hospital for Chronic Diseases has overcome innumerable difficulties, working actively to form a TB support group-the DOTS Club-with the aim of utilizing testimonials from recovered TB patients to raise the hopes and build the confidence of TB patients currently undergoing treatment, as well as countering the erroneous impressions that the general public has about TB. The hospital's head nurse Lin Hsiu-chin says that the DOTS Club, which was established in March of this year, currently has eight members. After receiving training on the physiology and psychology of tuberculosis, these DOTS emissaries will participate in TB prevention and awareness work.
Currently 36 years of age, Yang Chao-hung is one of the DOTS Club's "angels." When his tuberculosis became active, Yang was not yet 30, in the very prime of life. Who could have known that what seemed to be a cold that would not respond to any treatment, would turn out on detailed examination to be TB. This sudden blow shocked and frightened Yang. "I felt depressed, thinking life had no hope, and wanted to jump from the twelfth floor of the hospital," recalls Yang. Although family and friends did not desert him, at a time when therapeutic drugs were not as advanced as now, he had to swallow 20 pills every day, taking the medication for more than a year-it was truly an ordeal. After the disease was finally cured, no matter how busy with work he may be, Yang has been willing to make time to participate in the support group, providing encouragement to TB victims currently undergoing treatment.
Besides providing encouragement to TB victims, when confronted with a disease that has plagued humanity since time immemorial, people must have a proper understanding. "There is no need to be afraid," says Suo Jen, pointing out that helping each tuberculosis victim to receive proper treatment is the most important means of controlling its spread.
In fighting a battle, one must never underestimate the enemy. Confronted by tuberculosis, there is no cause for panic, but on the other hand one must not take its threat lightly. This is true for individuals, and true for disease control authorities.

Providing medication to patients personally and then observing as the patient ingests it is the principle behind DOTS (Directly Observed Treatment, Short-Course) programs, and is also an indispensable part of tuberculosis control efforts. (courtesy of Taipei's Hospital for Chronic Diseases)

Ancient communicable diseases resist eradication, while new ones emerge continually. Inhabitants of the modern world ought to have accurate knowledge, and maintain both physical and mental health, if they want to avoid contracting an infectious disease.

Tuberculosis prevention postage stamps issued by the National Tuberculosis Association. Such stamps were used both to raise funds for tuberculosis prevention efforts and to raise public awareness. (courtesy of the National Tuberculosis Association)

Tuberculosis prevention postage stamps issued by the National Tuberculosis Association. Such stamps were used both to raise funds for tuberculosis prevention efforts and to raise public awareness. (courtesy of the National Tuberculosis Association)




@List.jpg?w=522&h=410&mode=crop&format=webp&quality=80)



