The Wealth Gap in Medical Care
Chang Chiung-fang / photos Jimmy Lin / tr. by Scott Williams
November 2010

Chiang Tung-liang, dean of the College of Public Health at National Taiwan University, was aiming to do something important when he helped to plan Taiwan's National Health Insurance system: ensure that no one in Taiwan is medically disadvantaged.
Taiwan's NHI is now 15 years old. Are some still medically disadvantaged? Is there still a wealth gap in our healthcare system?
Though there is a relationship between the medically disadvantaged and the socioeconomically disadvantaged, there is more evidence to suggest that the wealth gap in medical care is not the key cause of health inequality. In fact, the wealth gap is deceptive in that higher healthcare expenditures do not equate to higher quality of care. In this era of "commodification" of healthcare, those of us who want to "buy back" our health need to recognize this fact, and need more and better data about our healthcare options.
"Taitung is just one hour away from Taipei by air," says Chiang Tung-liang, dean of the College of Public Health at National Taiwan University. "But, close as it is, Taitung has a mortality rate almost twice as high (9.45 vs. 5.94 per 1,000) and an average life expectancy that is nine years less than Taipei's." Chiang says that the current average life expectancy in Taitung is 73 years. By 1986, it had already reached 75 years in Taipei. In other words, the two cities aren't separated by a one-hour flight, but a chasm a full 25 years wide.

Are medical-device advances and higher-resolution imaging improving the public's health? Are life expectancies growing as a result? We need to find out.
Why is there such a large disparity in the health of the citizens of Taipei and Taitung?
"Health inequalities don't mean that individuals are in poor health," explains Chiang. "They are indicative of social inequities." In this respect, health inequities are much like wealth-poverty issues. Chiang explains that the spread of the Great Depression from the US to the rest of the world allowed people to recognize that no matter how hard they worked, individuals had difficulty escaping from poverty when social conditions were poor. The situation in healthcare is similar. When individuals in good health are subjected to difficult living circumstances, those circumstances give rise to stresses, risks and accidents that can ruin their health.
Chen Mei-shia, executive director of the Taiwan Association for Promoting Public Health and a professor of public health at National Cheng Kung University, says that research from around the world on the subject of health disparities shows a strong link between socioeconomic status and personal health: the lower people's socioeconomic standing, the poorer their health.
The situation is no different in Taiwan. A Ministry of the Interior survey of low-income persons found that 62% of low-income households had members who suffered from chronic or severe illnesses. It also found that the majority of low-income households were poor for reasons related to health issues.
"Regardless of the direction of causation," says Chen, "being socioeconomically disadvantaged and being health disadvantaged are closely linked." She cites Taiwan's indigenous peoples as an example, noting that their average life expectancy is 10 years less than that of Taiwan's Han Chinese. Given that 100 years ago the average life expectancies of both the Han Chinese and the indigenous peoples on Taiwan were less than 30 years, it is clear that genetics do not account for the present-day disparity.
Healthcare resources aren't the principal culprit, either. Chiang notes that Hualien County lags behind only the three special municipalities of Taipei, Taichung and Kaohsiung in terms of its healthcare resources. In fact, it has an average of one doctor per 450 residents versus just one per 831 in Taitung County. Yet, in spite of Hualien's enormous advantage in resources, the two counties have almost identical crude death rates: 9.26 per 1,000 in Hualien versus 9.45 per 1,000 in Taitung-the two highest in Taiwan. This strongly suggests that the health disadvantage of Taiwan's East Coast residents has some other cause.
"Most of the determinants for health fall outside the scope of medical care," says Chiang. "The most important is socioeconomic development." Chiang explains that cities' and counties' levels of socioeconomic development affect the standard of health their residents enjoy. The wealth gap between various cities and counties is also closely linked to health. (See table.)
The wealth gap between Taitung and Taipei offers compelling evidence. Taitung's household income is only half that of Taipei. Some 25% of Taitung's children grow up in poor households (low-income households are those with less than half the median income) compared to only 1% in Taipei. Children in these high-risk households are often raised by their grandparents and prepare their own meals, or they live alone. How can children who start life on such an unequal footing hope to have health equality later in their lives?
Steady improvements in medical technology mean that cataracts, nearsightedness, and presbyopia can now be treated with a single procedure. But patients need to think clearly about their specific needs and understand just what NHI will pay for.
Though health disparities don't arise out of medical care, we rely on the medical system to resolve them.
Chapter 3 of 2020 Healthy People, a white paper Chen produced for the Department of Health, argues that the "health behaviors" of low-education individuals are poorer across the board than those of high-education individuals. (Poor "health behaviors" include activities such as smoking and drinking to excess.) As a result, low-education individuals require more urgent and more frequent medical interventions. NHI data from recent years show that the poor make greater use of curative and palliative services such as outpatient care and surgery, and that the relatively well to do make greater use of preventive services, such as teeth cleanings and checkups.
Frequent and urgent medical care does not necessarily equate to health improvement. While Taiwan's NHI has alleviated the problems of illness causing poverty and poverty preventing access to care, it has not been able to eliminate the persistent health disparities between ethnic groups and between rural and urban areas, nor has it eliminated the inequities created by the wealth gap.
Minister of Health Yaung Chih-liang admits: "There's no such thing as a healthcare utopia. If one were to appear, it would be gone again in a flash."
The wealth gap in medical care does, however, affect healthcare choices and medical outcomes.
Chiang cites coronary heart disease, the number-two cause of death among Taiwan's adult population, as an example. NHI data show that socioeconomic status has a significant effect on whether patients receive bypass surgery and on the mortality rate among patients one year after surgery. Patients with higher levels of education are more likely to undergo surgery, yet have a significantly lower mortality rate one year after surgery.
Does the higher rate of surgery indicate that those of higher socioeconomic standing are more likely to suffer from the disease due to higher levels of work-related stress in their lives or greater amounts of overeating? Does it suggest earlier discovery and treatment of the disease? Does the lower death rate indicate that persons of higher socioeconomic standing receive better post-surgical care? Or that they are more likely to heed their doctors' advice and change their lifestyles? Though there has yet to be a deeper exploration of the causes, the wealth gap clearly correlates to different medical behaviors.
What's worrisome is that the Taiwan's NHI system doesn't treat medical services as a human right or social welfare, but as a product that must be bought. This has enabled the program to account for and respond to the government's fiscal position and the effectiveness of medical treatments, but has also given rise to a bizarre side effect: healthcare inequities that grow with the wealth gap.

In spite of our profusion of medical resources, some places still go wanting, revealing the need for a more nuanced policy effort. Here, the home care teama from Taitung's St. Mary's Hospital visits remote Taiyuan Village.
"The commodification of healthcare is the root of the problem," argues Chen. "The public is held captive by the healthcare system."
She views the world's healthcare delivery systems as "government-provided healthcare," "universal health insurance," or "diversified market-based health insurance" systems depending on how they provide and pay for medical services.
The UK, Denmark, Spain, and Sweden treat medical care as social welfare. That is, they have national health services wherein the government covers most health insurance costs and most healthcare providers are themselves government agencies.
Taiwan's system is similar to those of Germany, France, and Japan in that it uses social insurance to pay for medical care. While this ensures that most of the public has access to basic medical care and protects families from medical bankruptcies, the system is a public-private hybrid that is market-driven and profit-seeking.
Chen says that Taiwan's healthcare market is very profitable. This has resulted in a steady flow of private investment that has promoted years of growth in the healthcare system. As the market has become saturated, healthcare institutions have begun using a variety of methods to generate earnings. They do everything they can to "recruit" patients and stimulate demand in an effort to capture a larger share of the NHI pie. The result has been ever higher healthcare outlays. In 1995, when the NHI system was established, annual expenditures on healthcare in Taiwan were NT$50.7 billion. By 2008, they had risen to NT$788.5 billion, a 15-fold increase over 14 years. Meanwhile, the number of hospital beds in Taiwan has grown from nearly 40,000 30 years ago to more than 150,000 today.
Hospitals and treatment centers compete with one another to attract wealthy patients through their purchases of advanced medical devices like the da Vinci Surgical System, a robotic surgical system used for prostate and cardiac surgeries that incorporates high-resolution 3D imaging. Surgeries with the system are expensive, with the materials costs running to nearly NT$100,000 per operation. Taiwan also has the world's highest concentration of positron emission tomography (PET) scanners, which cost NT$32,000 per use.
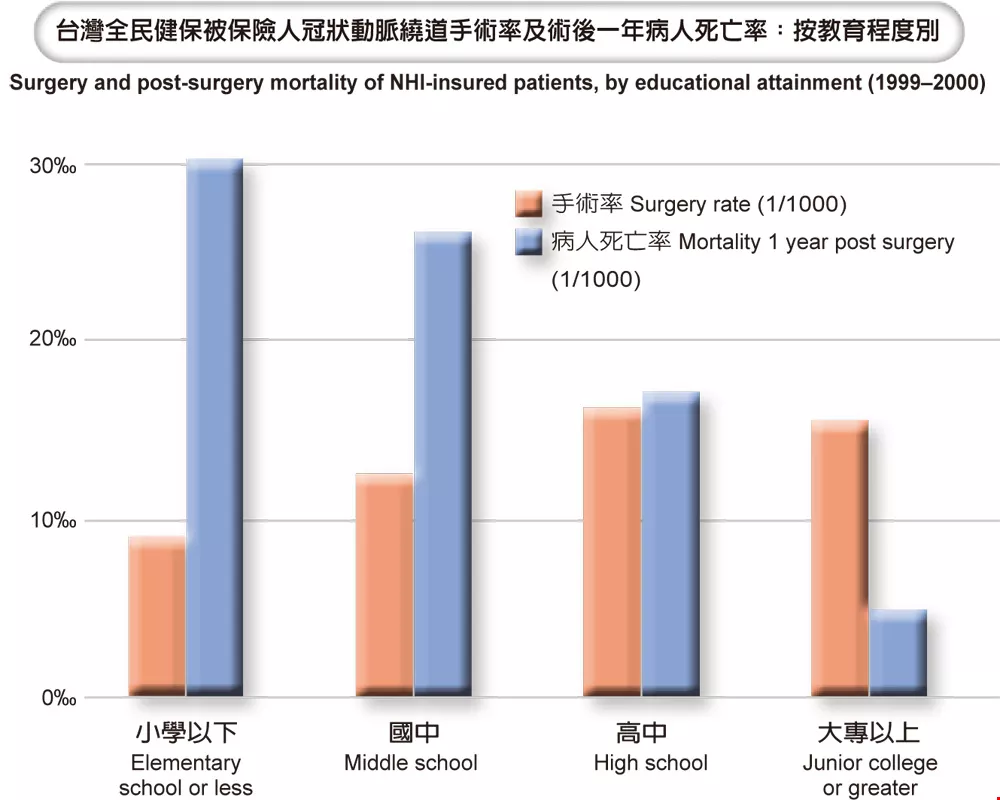
Surgery and post-surgery mortality of NHI-insured patients, by educational attainment
In a profit-oriented healthcare market, the healthcare fees the public pays will rise. Chen says that in 1980 healthcare costs accounted for 4.2% of Taiwanese household income. By 2008, they accounted for 14.6%, and the poorer the household, the heavier the burden.
In 2007 Taiwan's richest quintile spent 13% of household income on medical expenses, while our poorest quintile spent 22%.
To curb the massive growth in healthcare expenditures, the Bureau of National Health Insurance (BHNI) increased NHI premiums and increased the out-of-pocket costs to participants in the system (e.g. copayments increased to NT$360 at medical centers, NT$240 at regional hospitals, NT$80 at local hospitals, and NT$50 at clinics). The BNHI hoped in this way to encourage members of the public to be more conscientious in their use of medical resources. Officials didn't recognize that their seemingly reasonable proposal was misdirected and actually worsened income-related healthcare inequality.
Chen says that patients don't have the medical information they need to make sound judgments and choices. As a consequence, medical providers (i.e. doctors), not patients, are the principal decision makers when it comes the kind and amount of medical treatment. The result is large volumes of expensive, redundant, aggressive, and very likely ineffective treatments.
Moreover, Chiang says that currently just three out of every 10 emergency-room beds are set aside for NHI patients, leading to lines of patients lying on gurneys in emergency-room hallways even in public hospitals. The Taiwan Healthcare Reform Foundation (THRF) has cited the difficulty NHI patients face in getting a bed as the Taiwanese public's top healthcare complaint.
Under the Regulations Governing Examination of Medical Care Services for National Health Insurance Medical Care Institutions, public medical centers are supposed to reserve 65% of their beds for NHI patients and private medical centers 50%, but many institutions ignore the law. Eva Teng, spokesperson for the National Health Insurance Civic Surveillance Alliance, reveals that Taiwan's top public hospital, National Taiwan University Hospital, keeps less than 60% of its beds for NHI patients.
With beds hard to come by, members of the public can either wait for a space in a ward containing three to six beds, or pay thousands of NT dollars extra per day for a private room. This cost explains why wealthy patients spend far more time in the hospital than poor patients (11.5 days versus 1.5 days per year) though they visit less frequently, and why the disparity in the length of hospital stays is growing.

Seeking to draw wealthy clients in for exams, preventive care provider HealthConn contracted with the nearby five-star Sheraton Hotel and a nutritionist to provide the kind of healthy meals that make patients feel at home.
To patients, medical services are an "intermediate product" rather than their ultimate objective. They naturally continue to seek medical care until they achieve that objective: a return to good health.
Recognizing the power of patients' desires for good health, medical institutions have not only been pursuing a large piece of the NHI pie, but also encouraging patients to spend money out of pocket to receive "even better" care. As a result, the ratio of out-of-pocket expenses to covered expenses has been rising steadily in recent years.
In early October, the THRF published a survey showing that more than 46% of the public paid medical fees over and above their copayments and coinsurance costs.
According to the BNHI website, medical centers most frequently ask patients to pay out of pocket for IV drips. Other common items include disposable medical products (e.g. single-use ear-temperature-gun sheaths, enema syringes, catheters, and drainage bags), patient-controlled administration of analgesics, hyperbaric oxygen therapy, and PET scans.
Close scrutiny shows most out-of-pocket expenses to be superfluous, though they can, in a few limited circumstances, be crucial.
The contrast agents used with some imaging technologies offer an excellent example.
In recent years, PET scans have vaulted to the top of the BNHI's top 10 examination procedures. The scans, which are touted for their ability to "see through the whole body," require the injection of a contrast agent. Generally speaking, NHI will pay for the use of the traditional ionic contrast agent, but this agent can cause nausea, vomiting, and even allergic reactions (at a 4-12% rate). To protect high-risk groups, BNHI will pay for the use of a non-ionic contrast agent for patients who meet any one of nine criteria, including impaired kidney function and major organ failure. But there's a catch: until recently the exception applied to a maximum of only 10% of examinations. Hospitals used this ceiling as an excuse to demand that patients themselves pay NT$1500 for the injection of the non-ionic contrast agent, thereby fattening their bottom lines.
In one case, a Mr. Lin, an 80-year-old man with poor kidney function, was asked to pay for the non-ionic injection. Lacking the money to pay the extra fee, he took a chance on the traditional ionic contrast agent, had an allergic reaction to it, and died.
In the wake of his unfortunate death, the Department of Health last year announced that it would eliminate the 10% cap and would pay for the use of the non-ionic agent for any patient that met one of the nine criteria. It also forbade hospitals from deceiving or rejecting patients.
Other dilemmasExpensive new anticancer drugs similarly fall into the out-of-pocket category. Should you take them or not? Are they worth a roll of the dice? Such questions place patients and their families squarely on the horns of a dilemma.
Sheen Mao-ting, director of BNHI's Medical Review and Pharmaceutical Benefits Division, says cancer treatment is rife with out-of-pocket expenses, especially when you get into the realm of tailor-made targeted drugs. Trastuzumab, used to treat certain varieties of breast cancer, is a case in point. A year's supply of the medication costs an average of NT$700-800,000. At present, these kinds of incredibly expensive experimental drugs can only delay death; they don't cure the cancer. From the BNHI's standpoint, their costs outweigh their benefits, and it won't pay for them. This leaves patients and their families to decide for themselves whether to use (and shoulder the costs of) such treatments.
Out-of-pocket expenses also include "off-label" uses of medications. For example, there are currently no drugs specifically aimed at the treatment of colorectal cancer, and doctors frequently administer breast-cancer drugs to patients. The effectiveness of off-label uses is largely a matter of luck, so NHI won't pay for them, leaving patients to pay their entire cost themselves.
Sometimes out-of-pocket expenses aren't a matter of life and death, but simply of how much a patient can bear. Pain medications are a case in point.
Everyone who has had surgery knows that post-surgical pain from the wound can be hard to bear. Now that we have patient-controlled administration of pain medications, patients are able to press a button to administer analgesics any time they feel pain. Though this is great for patients, its costs them NT$3,000-7,000 out of pocket depending on their course of treatment.
But patient-controlled administration of analgesics isn't the only way to go. NHI pays for both the oral administration and the injection of painkillers, but hospitals are reluctant to provide adequate doses of the drugs in this manner.
Medical pillage?In addition to encouraging patients to pay out of pocket for "better" care than NHI provides, some medical facilities simply invent their own out-of-pocket expenses. As a result, the public at large is coming to view hospitals as money pits and the economically disadvantaged are becoming even less willing to visit them unless they absolutely must.
A THRF survey of Taiwan's 25 counties and metropolises shows that "medical looting" makes "products" of services that had previously been free of charge and invents "special perks" that are easily tiered by price. For example, medical facilities now charge NT$100 to check medical records, NT$250-1000 to make an appointment with a specific outpatient clinician, NT$10-30,000 to get a specific surgeon for an operation, NT$200 to request to be squeezed into the schedule of a doctor who has already seen his or her allotted number of patients for the day, and NT$500 if a consultation goes beyond 15 minutes. In addition, hospitals are now charging NT$300-1,000 to change beds (e.g. from a non-NHI bed to an NHI bed), NT$150 to jump the queue to see a doctor early, and NT$100 to grind up medications. According to the THRF's study, the last three charges have long been explicitly banned by the health bureaus of each of Taiwan's counties and municipalities.
Some of these items are more than a little arbitrary and even dodgy in their implementation. For example, creating a disk backup of medical records costs NT$200 at some hospitals and NT$1,000 at others, a difference of 500%. Charging a fee to check medical records is banned in 18 counties and municipalities and "recommend against" in a further four. Charging a fee to see a specific doctor is likewise banned in 17 counties and municipalities, but permitted in five others.
Patients are already frightened by their illnesses. Arbitrary billing standards make matters worse, and leave patients feeling that going to the hospital means getting fleeced.
The limits of careIn the commoditized healthcare market, there's a constant parade of new products. This confuses people, who don't know what to choose. Given that there are limits to medical care, it's worth considering whether the "good, or better?" direction in which the medical system is so vigorously moving is correct.
Chiang says that over the last 100 years, the average life expectancy of Taiwanese has grown by 50 years. It's an amazing achievement, on a par with our economic miracle. But in recent years, there has been a sharp decline in marginal improvements. Most of the 120,000 people who die every year have simply reached the end of their days. Fewer than 20% could have been saved by better, more extreme medical procedures.
In other words, medical care can improve the quality of life, but has reached the limits of its ability to extend life.
Given that the use by patients at the top of the socioeconomic pyramid of every available treatment will do little to extend their lives, Chiang sincerely urges that we utilize more of our resources to shrink the health disparities between rich and poor, and strengthen programs to encourage people to lose weight, stop smoking and quit drinking. Health programs such as anti-drug advocacy and the construction of public health information networks are, in his view, the only way to reduce pervasive health disparities and maximize the effectiveness of modern health care.
"Taiwan spends NT$800 billion on healthcare every year, but 92% of that amount is on treatment. Preventive care accounts for only 3% of spending," says Chen, who strongly urges that we turn those numbers around.
It seems that if we are to end wealth-related health disparities and create genuine health equality, we need to put the brakes on the commodification of healthcare and rethink our allocation of healthcare resources. Instead of putting all our resources into saving those who are drowning, we need to keep people from falling into the river in the first place. This is the principle we should be applying to resolving the wealth gap in medical care and our health inequalities.







